

Review article: Update on current and emergent data on hepatopulmonary syndrome
- PMID: 29599604
- PMCID: PMC5871824
- DOI: 10.3748/wjg.v24.i12.1285
Review article: Update on current and emergent data on hepatopulmonary syndrome
Abstract
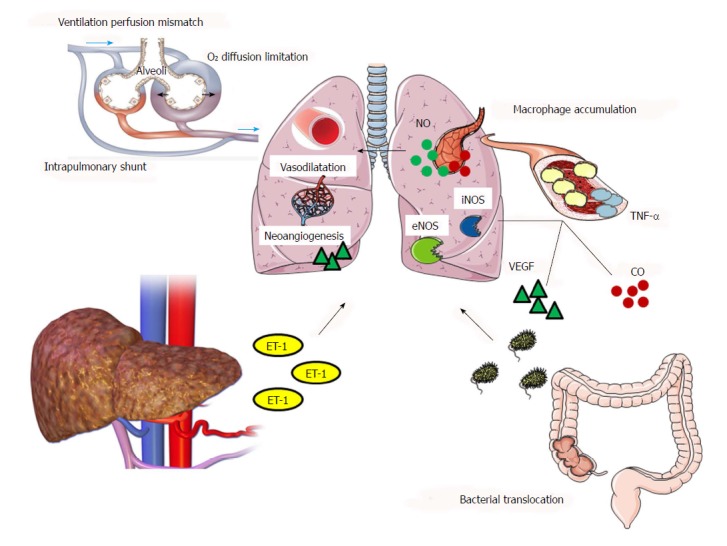
Hepatopulmonary syndrome (HPS) is a frequent pulmonary complication of end-stage liver disease, characterized by impaired arterial oxygenation induced by intrapulmonary vascular dilatation. Its prevalence ranges from 4% to 47% in patients with cirrhosis due to the different diagnostic criteria applied among different studies. Nitric oxide overproduction and angiogenesis seem to be the hallmarks of a complicated pathogenetic mechanism, leading to intrapulmonary shunting and ventilation-perfusion mismatch. A classification of HPS according to the severity of hypoxemia has been suggested. Contrast-enhanced echocardiography represents the gold standard method for the detection of intrapulmonary vascular dilatations which is required, in combination with an elevated alveolar arterial gradient to set the diagnosis. The only effective treatment which can modify the syndrome's natural history is liver transplantation. Although it is usually asymptomatic, HPS imparts a high risk of pretransplantation mortality, independently of the severity of liver disease, while there is variable data concerning survival rates after liver transplantation. The potential of myocardial involvement in the setting of HPS has also gained increasing interest in recent research. The aim of this review is to critically approach the existing literature of HPS and emphasize unclear points that remain to be unraveled by future research.
Keywords: Contrast echocardiography; Hepatopulmonary syndrome; Liver cirrhosis; Liver transplantation; Portal hypertension.
Conflict of interest statement
Conflict-of-interest statement: The authors have no financial or other conflicts of interest related to the submitted manuscript to declare.
Figures
References
-
- Kiafar C, Gilani N. Hepatic hydrothorax: current concepts of pathophysiology and treatment options. Ann Hepatol. 2008;7:313–320. - PubMed
-
- Fussner LA, Krowka MJ. Current Approach to the Diagnosis and Management of Portopulmonary Hypertension. Curr Gastroenterol Rep. 2016;18:29. - PubMed
-
- Rodríguez-Roisin R, Krowka MJ, Hervé P, Fallon MB; ERS Task Force Pulmonary-Hepatic Vascular Disorders (PHD) Scientific Committee. Pulmonary-Hepatic vascular Disorders (PHD) Eur Respir J. 2004;24:861–880. - PubMed
-
- Kennedy TC, Knudson RJ. Exercise-aggravated hypoxemia and orthodeoxia in cirrhosis. Chest. 1977;72:305–309. - PubMed
-
- Hoffbauer FW, Rydell R. Multiple pulmonary arteriovenous fistulas in juvenile cirrhosis. Am J Med. 1956;21:450–460. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
