

Successful combination of direct antiviral agents in liver-transplanted patients with recurrent hepatitis C virus
- PMID: 29599610
- PMCID: PMC5871830
- DOI: 10.3748/wjg.v24.i12.1353
Successful combination of direct antiviral agents in liver-transplanted patients with recurrent hepatitis C virus
Abstract
Aim: To analyze the safety and efficiency of direct-acting antiviral (DAA) regimens in liver-transplanted patients with hepatitis C virus (HCV) reinfection.
Methods: Between January 2014 and December 2016, 39 patients with HCV reinfection after liver transplantation were treated at our tertiary referral center with sofosbuvir (SOF)-based regimens, including various combinations with interferon (IFN), daclatasvir (DAC), simeprivir (SIM) and/or ledipasvir (LDV). Thirteen patients were treated with SOF + IFN ± RBV. Ten patients were treated with SOF + DAC ± RBV. Fiveteen patients were treated with fixed-dose combination of SOF + LDV ± RBV. One patient was treated with SOF + SIM + RBV. Three patients with relapse were retreated with SOF + LDV + RBV. The treatment duration was 12-24 wk in all cases. The decision about the HCV treatment was made by specialists at our transplant center, according to current available or recommended medications.
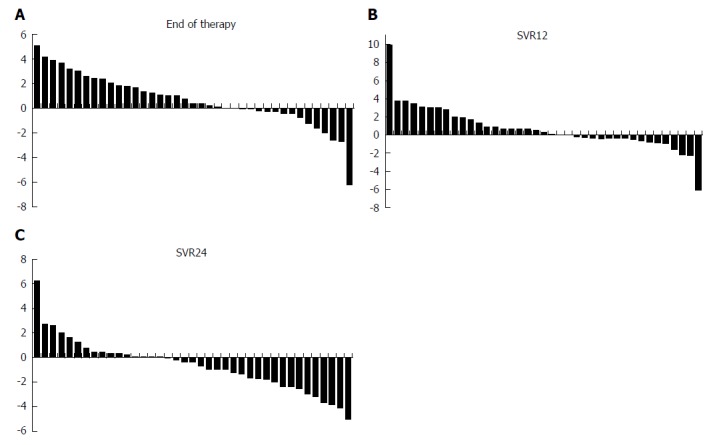
Results: The majority of patients were IFN-experienced (29/39, 74.4%) and had a history of hepatocellular carcinoma (26/39, 66.7%) before liver transplantation. Sustained virological response at 12 wk (SVR12) was achieved in 10/13 (76.9%) of patients treated with SOF + IFN ± RBV. All patients with relapse were treated with fixed-dose combination of SOF + LDV + RBV. Patients treated with SOF + DAC + RBV or SOF + LDV + RBV achieved 100% SVR12. SVR rates after combination treatment with inhibitors of the HCV nonstructural protein (NS)5A and NS5B for 24 wk were significantly higher, as compared to all other therapy regimens (P = 0.007). Liver function was stable or even improved in the majority of patients during treatment. All antiviral therapies were safe and well-tolerated, without need of discontinuation of treatment or dose adjustment of immunosuppression. No serious adverse events or any harm to the liver graft became overt. No patient experienced acute cellular rejection during the study period.
Conclusion: Our cohort of liver-transplanted patients achieved high rates of SVR12 after a 24-wk course of treatment, especially with combination of NS5A and NS5B inhibitors.
Keywords: Direct acting antivirals; Hepatitis C virus; Liver transplantation; Recurrence; Sustained virological response.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflicts of interest.
Figures
References
-
- Goldberg D, Ditah IC, Saeian K, Lalehzari M, Aronsohn A, Gorospe EC, Charlton M. Changes in the Prevalence of Hepatitis C Virus Infection, Nonalcoholic Steatohepatitis, and Alcoholic Liver Disease Among Patients With Cirrhosis or Liver Failure on the Waitlist for Liver Transplantation. Gastroenterology. 2017;152:1090–1099.e1. - PMC - PubMed
-
- Lohmann V, Körner F, Koch J, Herian U, Theilmann L, Bartenschlager R. Replication of subgenomic hepatitis C virus RNAs in a hepatoma cell line. Science. 1999;285:110–113. - PubMed
-
- Bartenschlager R, Lohmann V, Penin F. The molecular and structural basis of advanced antiviral therapy for hepatitis C virus infection. Nat Rev Microbiol. 2013;11:482–496. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
