

Outcomes of transconjunctival sutureless 27-gauge vitrectomy for vitreoretinal diseases
- PMID: 29600174
- PMCID: PMC5861230
- DOI: 10.18240/ijo.2018.03.10
Outcomes of transconjunctival sutureless 27-gauge vitrectomy for vitreoretinal diseases
Abstract
Aim: To evaluate the safety and efficacy profile of 27-gauge (27G) pars plana vitrectomy (PPV) for the treatment of various vitreoretinal diseases.
Methods: The clinical outcomes of 61 eyes (58 patients) with various vitreoretinal diseases following 27G PPV were retrospectively reviewed.
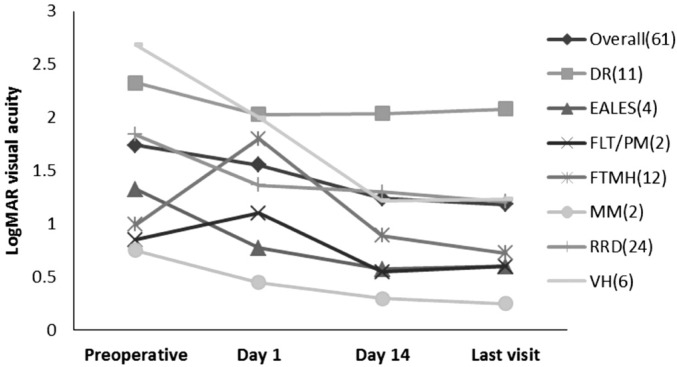
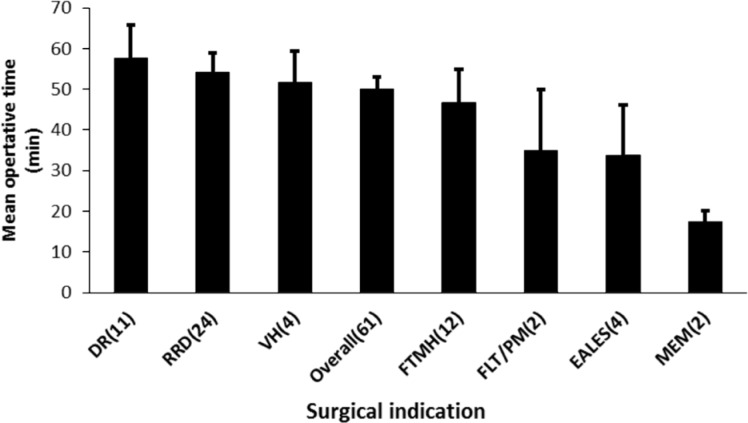
Results: Surgical indications included rhegmatogenous retinal detachment (n=24), full-thickness macular hole (n=12), diabetic retinopathy (n=11), vitreous hemorrhage (n=6), Eales disease (n=4), pathological myopia-related vitreous floater (n=2), and macular epiretinal membrane (n=2). The mean follow-up was 166.4±61.3d (range 98-339d). The mean logMAR best-corrected visual acuity (BCVA) improved from 1.7±1.1 [0.02 decimal visual acuity (VA) equivalent] preoperatively to 1.2±1.0 (0.06 decimal VA equivalent) at the last postoperative visit (P<0.001). The mean operative time was 49.9min. With the exception of complicated cataract in one eye, no intraoperative complications were encountered. No case required conversion to conventional 20-, 23- or 25G instrumentation in all surgical maneuvers except for silicone oil infusion, which required a 25G oil injection syringe. Postoperative complications included transient ocular hypertension, vitreous hemorrhage, persistent intraocular pressure elevation, subconjunctival oil leakage, and recurrent retinal detachment. No cases of hypotony, endophthalmitis, and sclerotomy-related tears were observed.
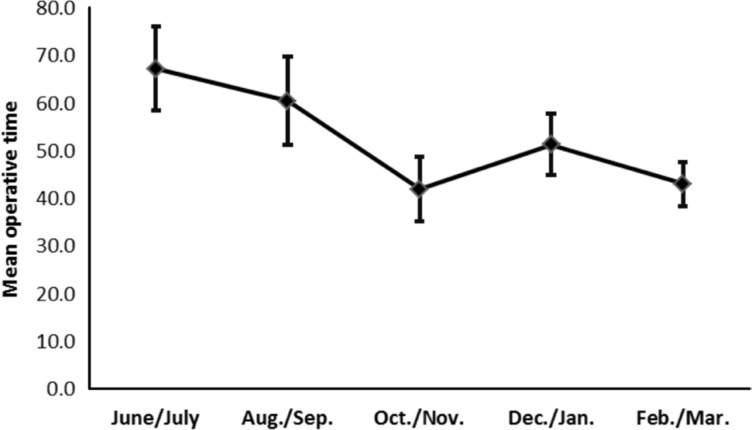
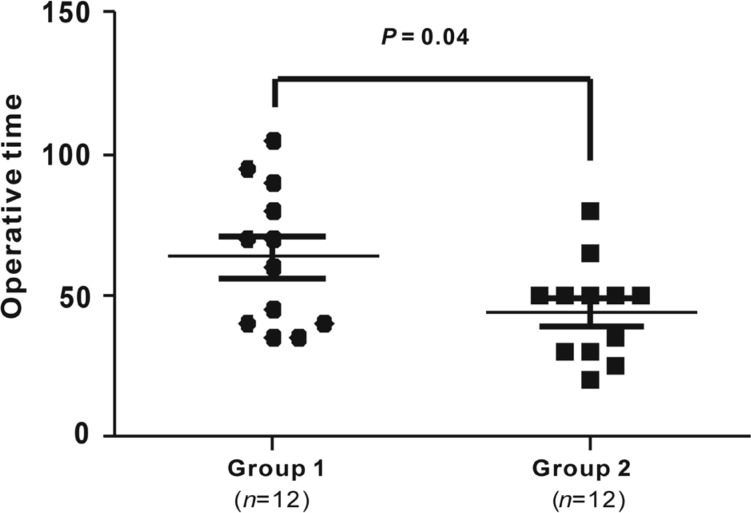
Conclusion: The current results suggest that 27G PPV system is a safe and effective treatment for various vitreoretinal diseases. When learning to perform 27G PPV, surgeons may encounter a learning curve and should gradually expand surgical indications from easy to pathologically complicated cases.
Keywords: 27-gauge; par plana vitrectomy; vitreoretinal disease.
Figures
References
-
- Machemer R, Buettner H, Norton EW, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(4):813–820. - PubMed
-
- Fujii GY, De Juan E, Jr, Humayun MS, Pieramici DJ, Chang TS, Awh C, Ng E, Barnes A, Wu SL, Sommerville DN. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology. 2002;109(10):1807–1812. - PubMed
-
- Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina. 2005;25(2):208–211. - PubMed
-
- Rizzo S, Genovesi-Ebert F, Murri S, Belting C, Vento A, Cresti F, Manca ML. 25-gauge, sutureless vitrectomy and standard 20-gauge pars plana vitrectomy in idiopathic epiretinal membrane surgery: a comparative pilot study. Graefes Arch Clin Exp Ophthalmol. 2006;244(4):472–479. - PubMed
-
- Scott IU, Flynn HW, Jr, Dev S, Shaikh S, Mittra RA, Arevalo JF, Kychenthal A, Acar N. Endophthalmitis after 25-gauge and 20-gauge pars plana vitrectomy: incidence and outcomes. Retina. 2008;28(1):138–142. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous