

Four-year antibody persistence and response to a booster dose of a pentavalent MenABCWY vaccine administered to healthy adolescents and young adults
- PMID: 29601256
- PMCID: PMC5989907
- DOI: 10.1080/21645515.2018.1457595
Four-year antibody persistence and response to a booster dose of a pentavalent MenABCWY vaccine administered to healthy adolescents and young adults
Abstract
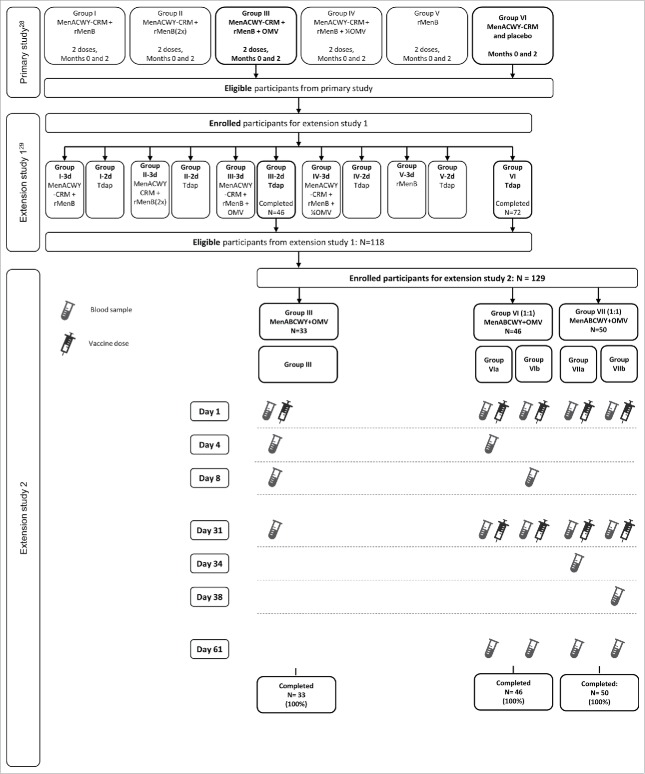
This open-label, multicenter extension study (NCT02451514) assessed persistence of Neisseria meningitidis serogroups ABCWY antibodies 4 years after primary vaccination. Adolescents and young adults who previously received 2 doses of MenABCWY+OMV (Group III), 1 dose of MenACWY-CRM (Group VI), or newly-recruited vaccine-naïve participants (Group VII) were administered 1 (Group III) or 2 doses (Groups VI and VII) of MenABCWY+OMV, 1 month apart. Immunogenicity was assessed by human serum bactericidal assay (hSBA). Safety and reactogenicity were also evaluated. Percentages of participants with hSBA titers ≥8 (serogroups ACWY), ≥5 (serogroup B) and hSBA geometric mean titers (GMTs) were evaluated in all 129 enrolled participants (Group III: 33; Group VI: 46; Group VII: 50). Anti-ACWY antibody concentrations waned over 4 years post-vaccination, but remained above pre-vaccination concentrations. Similarly, levels of antibodies against serogroup B test strains also waned over 4 years post-vaccination, but remained above pre-vaccination concentrations for some strains. MenABCWY+OMV booster induced a robust anamnestic anti-ACWY response in Group III and VI and a good response against serogroup B test strains (≥82%) in Group III. In serogroup B-naïve participants (Groups VI and VII), anti-B responses to 2 doses of MenABCWY+OMV were less homogenous and lower than in Group III. MenABCWY+OMV was reactogenic, but well-tolerated. No safety concerns were identified. These findings indicate that although antibodies against N. meningitidis serogroups ABCWY waned over 4 years post-vaccination, exposure to a MenABCWY+OMV booster dose elicits an anamnestic response in adolescents previously exposed to the same or another multivalent meningococcal vaccine.
Keywords: MenABCW; MenACWY; antibody persistence; booster dose; meningococcal vaccine.
Figures


References
-
- European Centre for Disease Prevention and Control Surveillance of invasive bacterial diseases in Europe 2007. [accessed February14, 2018]. http://www.ecdc.europa. eu/en/publications/Publications/101011_SUR_Surve....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical