

Predicting adverse hemodynamic events in critically ill patients
- PMID: 29601321
- PMCID: PMC6007856
- DOI: 10.1097/MCC.0000000000000496
Predicting adverse hemodynamic events in critically ill patients
Abstract
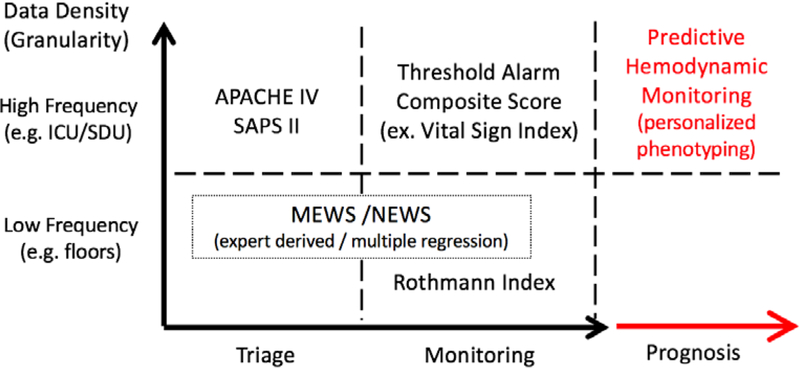
Purpose of review: The art of predicting future hemodynamic instability in the critically ill has rapidly become a science with the advent of advanced analytical processed based on computer-driven machine learning techniques. How these methods have progressed beyond severity scoring systems to interface with decision-support is summarized.
Recent findings: Data mining of large multidimensional clinical time-series databases using a variety of machine learning tools has led to our ability to identify alert artifact and filter it from bedside alarms, display real-time risk stratification at the bedside to aid in clinical decision-making and predict the subsequent development of cardiorespiratory insufficiency hours before these events occur. This fast evolving filed is primarily limited by linkage of high-quality granular to physiologic rationale across heterogeneous clinical care domains.
Summary: Using advanced analytic tools to glean knowledge from clinical data streams is rapidly becoming a reality whose clinical impact potential is great.
Figures

References
-
- Harris CRS.Galen’s Pulse-Lore The Heart and the Vascular System in Ancient Greek Medicine, from Alcmaeon to Galen. Oxford, UK: Clarendon Press; 1973.
-
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Critical care medicine 1985; 13: 818-829. - PubMed
-
- Moreno RP, Metnitz PG, Almeida E, Jordan B, Bauer P, Campos RA, Iapichino G, Edbrooke D, Capuzzo M, Le Gall JR. SAPS 3--From evaluation of the patient to evaluation of the intensive care unit. Part 2: Development of a prognostic model for hospital mortality at ICU admission. Intensive care medicine 2005; 31: 1345-1355. - PMC - PubMed
-
- Zimmerman JE, Kramer AA, McNair DS, Malila FM. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today's critically ill patients. Critical care medicine 2006; 34: 1297-1310. - PubMed
-
- Higgins TL, Teres D, Copes WS, Nathanson BH, Stark M, Kramer AA. Assessing contemporary intensive care unit outcome: an updated Mortality Probability Admission Model (MPM0-III). Critical care medicine 2007; 35: 827-835. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
