

Are Age and Patient Gender Associated With Different Rates and Magnitudes of Clinical Improvement After Reverse Shoulder Arthroplasty?
- PMID: 29601384
- PMCID: PMC6263575
- DOI: 10.1007/s11999.0000000000000270
Are Age and Patient Gender Associated With Different Rates and Magnitudes of Clinical Improvement After Reverse Shoulder Arthroplasty?
Abstract
Background: An improved understanding of how gender differences and the natural aging process are associated with differences in clinical improvement in outcome metric scores and ROM measurements after reverse total shoulder arthroplasty (rTSA) may help physicians establish more accurate patient expectations for reducing postoperative pain and improving function.
Questions/purposes: (1) Is gender associated with differences in rTSA outcome scores like the Simple Shoulder Test (SST), the UCLA Shoulder score, the American Shoulder and Elbow Surgeons (ASES) Shoulder score, the Constant Shoulder score, and the Shoulder Pain and Disability Index (SPADI) and ROM? (2) Is age associated with differences in rTSA outcome scores and ROM? (3) What factors are associated with the combined interaction effect between age and gender? (4) At what time point during recovery does most clinical improvement occur, and when is full improvement reached?
Methods: We quantified and analyzed the outcomes of 660 patients (424 women and 236 men; average age, 72 ± 8 years; range, 43-95 years) with cuff tear arthropathy or osteoarthritis and rotator cuff tear who were treated with rTSA by 13 shoulder surgeons from a longitudinally maintained international database using a linear mixed effects statistical model to evaluate the relationship between clinical improvements and gender and patient age. We used five outcome scoring metrics and four ROM assessments to evaluate clinical outcome differences.
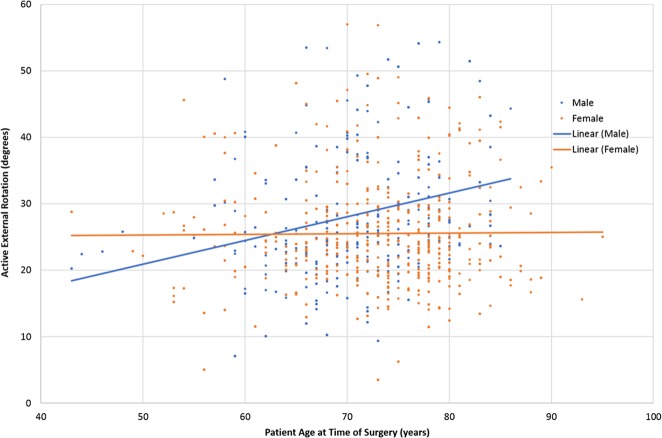
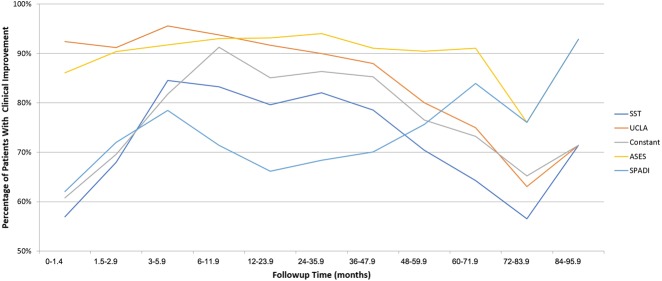
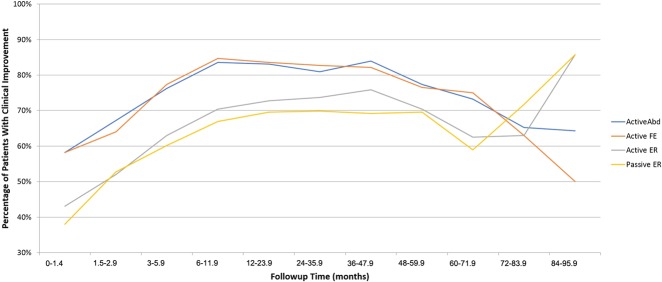
Results: When controlling for age, men had better SST scores (mean difference [MD] = 1.41 points [95% confidence interval {CI}, 1.07-1.75], p < 0.001), UCLA scores (MD = 1.76 [95% CI, 1.05-2.47], p < 0.001), Constant scores (MD = 6.70 [95% CI, 4.80-8.59], p < 0.001), ASES scores (MD = 7.58 [95% CI, 5.27-9.89], p < 0.001), SPADI scores (MD = -12.78 [95% CI, -16.28 to -9.28], p < 0.001), abduction (MD = 5.79° [95% CI, 2.74-8.84], p < 0.001), forward flexion (MD = 7.68° [95% CI, 4.15-11.20], p < 0.001), and passive external rotation (MD = 2.81° [95% CI, 0.81-4.8], p = 0.006). When controlling for gender, each 1-year increase in age was associated with an improved ASES score by 0.19 points (95% CI, 0.04-0.34, p = 0.011) and an improved SPADI score by -0.29 points (95% CI, -0.46 to 0.07, p = 0.020). However, each 1-year increase in age was associated with a mean decrease in active abduction by 0.26° (95% CI, -0.46 to 0.07, p = 0.007) and a mean decrease of forward flexion by 0.39° (95% CI, -0.61 to 0.16, p = 0.001). A combined interaction effect between age and gender was found only with active external rotation: in men, younger age was associated with less active external rotation and older age was associated with more active external rotation (β0 [intercept] = 11.029, β1 [slope for age variable] = 0.281, p = 0.009). Conversely, women achieved no difference in active external rotation after rTSA, regardless of age at the time of surgery (β0 [intercept] = 34.135, β1 [slope for age variable] = -0.069, p = 0.009). Finally, 80% of patients achieved full clinical improvement as defined by a plateau in their outcome metric score and 70% of patients achieved full clinical improvement as defined by a plateau in their ROM measurements by 12 months followup regardless of gender or patient age at the time of surgery with most improvement occurring in the first 6 months after rTSA.
Conclusions: Gender and patient age at the time of surgery were associated with some differences in rTSA outcomes. Men had better outcome scores than did women, and older patients had better outcome scores but smaller improvements in function than did younger patients. These results demonstrate rTSA outcomes differ for men and women and for different patient ages at the time of surgery, knowledge of these differences, and also the timing of improvement plateaus in outcome metric scores and ROM measurements can both improve the effectiveness of patient counseling and better establish accurate patient expectations after rTSA.
Level of evidence: Level III, therapeutic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Are Age and Patient Gender Associated With Different Rates and Magnitudes of Clinical Improvement After Reverse Shoulder Arthroplasty?Clin Orthop Relat Res. 2018 Jun;476(6):1274-1275. doi: 10.1097/01.blo.0000533613.25243.1c. Clin Orthop Relat Res. 2018. PMID: 29698306 Free PMC article. No abstract available.
References
-
- Bates D, Maechler M, Bolker B, Walker S. Fitting linear mixed-effects models using lme4. J Stat Softw. 2015;67:1–48.
-
- Boileau P, Watkinson D, Hatzidakis AM, Hovorka I. Neer Award 2005: The Grammont reverse shoulder prosthesis: results in cuff tear arthritis, fracture sequelae, and revision arthroplasty. J Shoulder Elbow Surg. 2006;15:527–540. - PubMed
-
- Frankle M, Siegal S, Pupello D, Saleem A, Mighell M, Vasey M. The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency. A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am. 2005;87:1697–1705. - PubMed
-
- Henn RF, 3rd, Ghomrawi H, Rutledge JR, Mazumdar M, Mancuso CA, Marx RG. Preoperative patient expectations of total shoulder arthroplasty. J Bone Joint Surg Am. 2011;93:2110–2115. - PubMed
-
- Holm S. A simple sequentially rejective multiple test procedure. Scand J Stat. 1979;6:65–70.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
