

HMGB1/IL-1β complexes in plasma microvesicles modulate immune responses to burn injury
- PMID: 29601597
- PMCID: PMC5877880
- DOI: 10.1371/journal.pone.0195335
HMGB1/IL-1β complexes in plasma microvesicles modulate immune responses to burn injury
Abstract
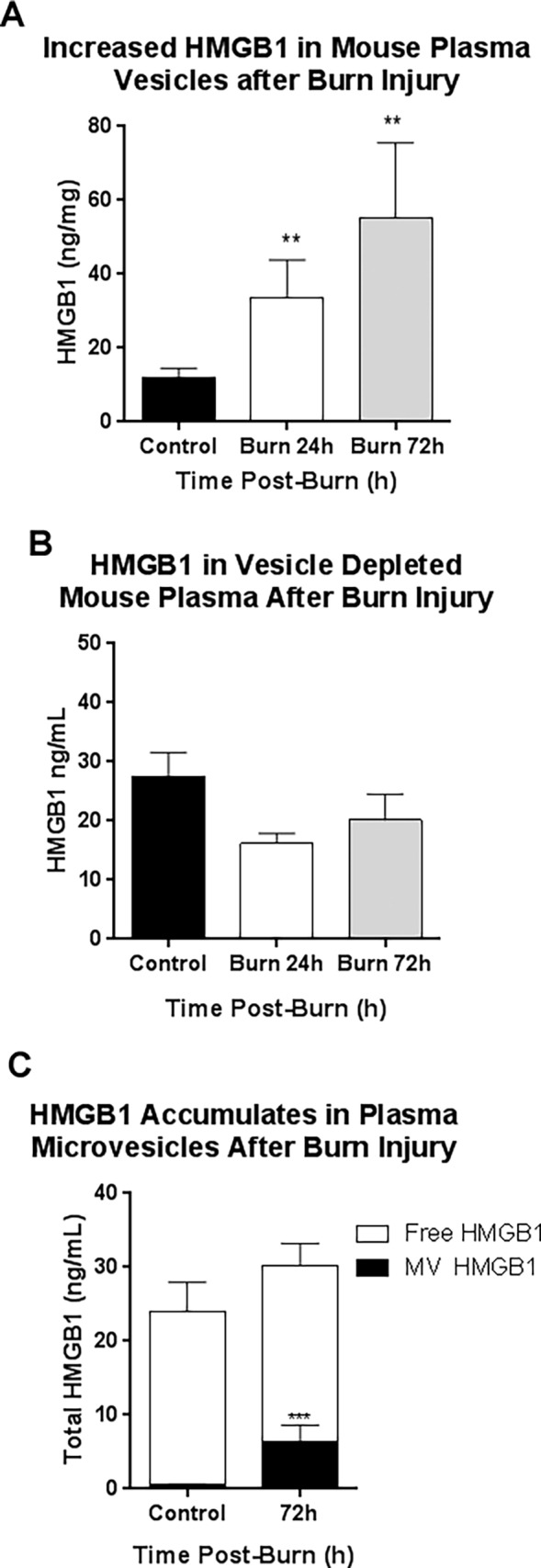
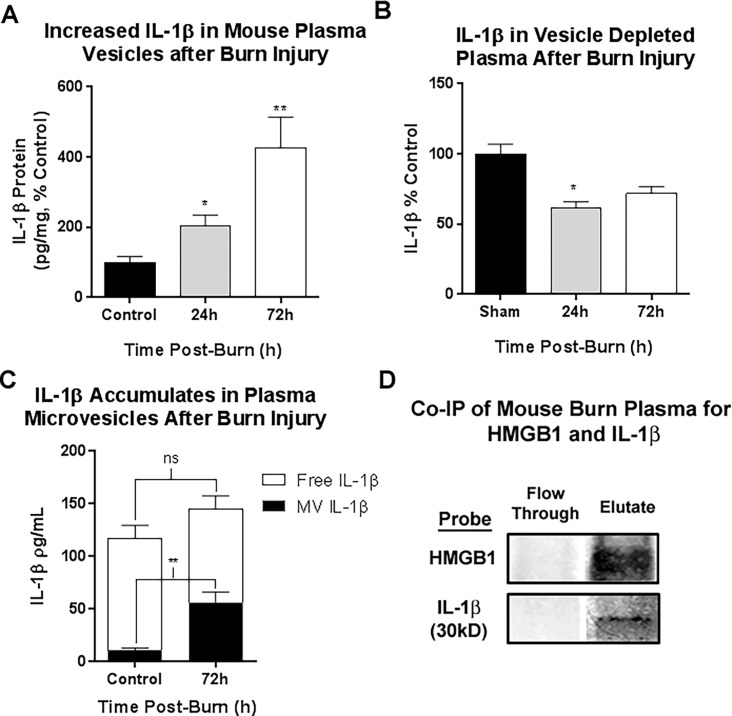
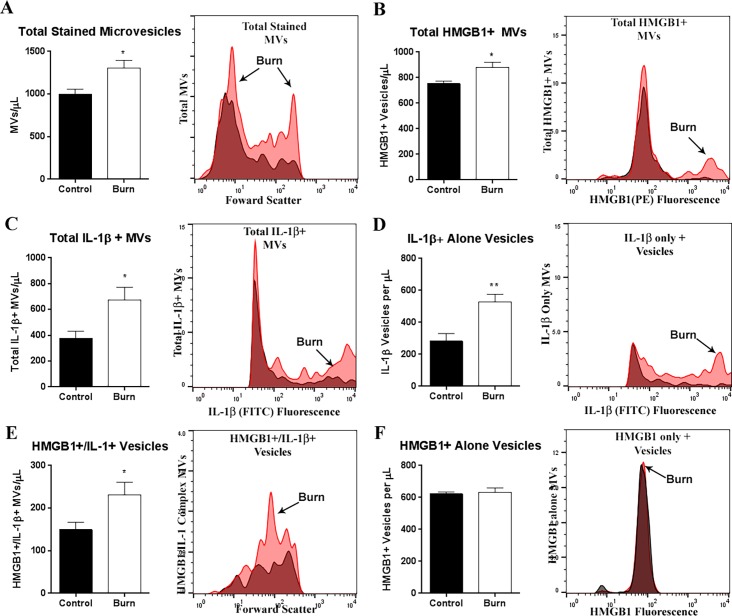
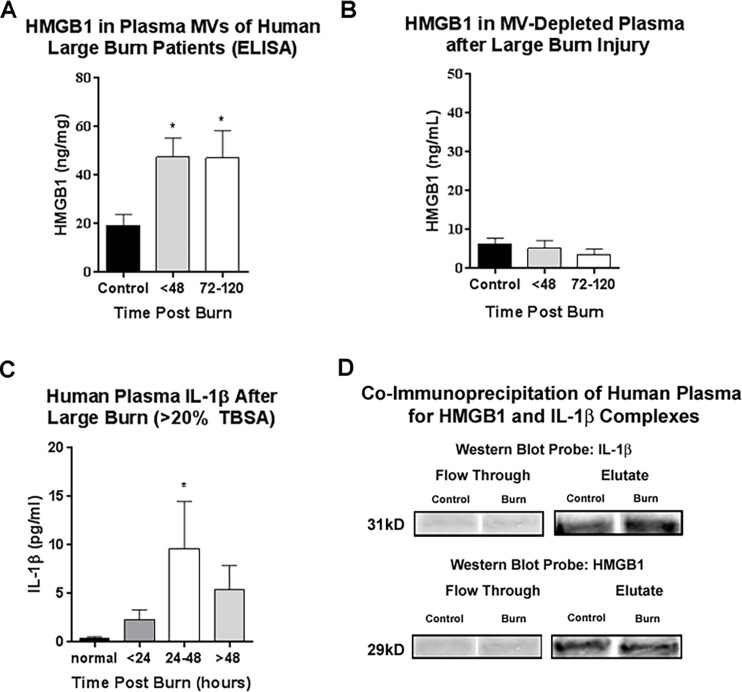
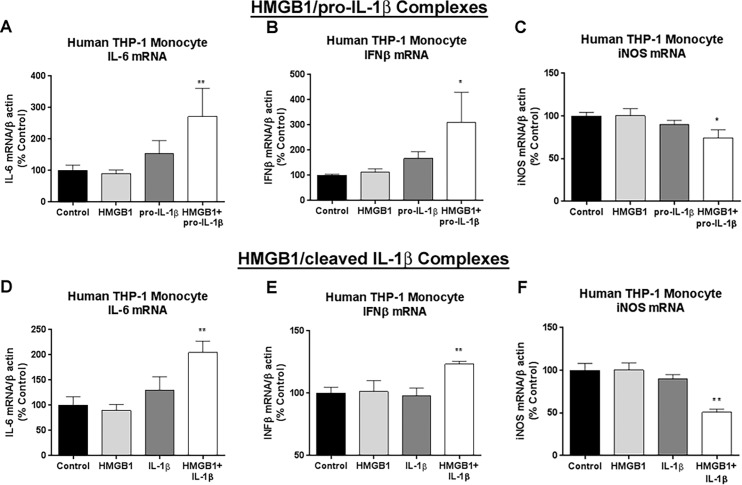
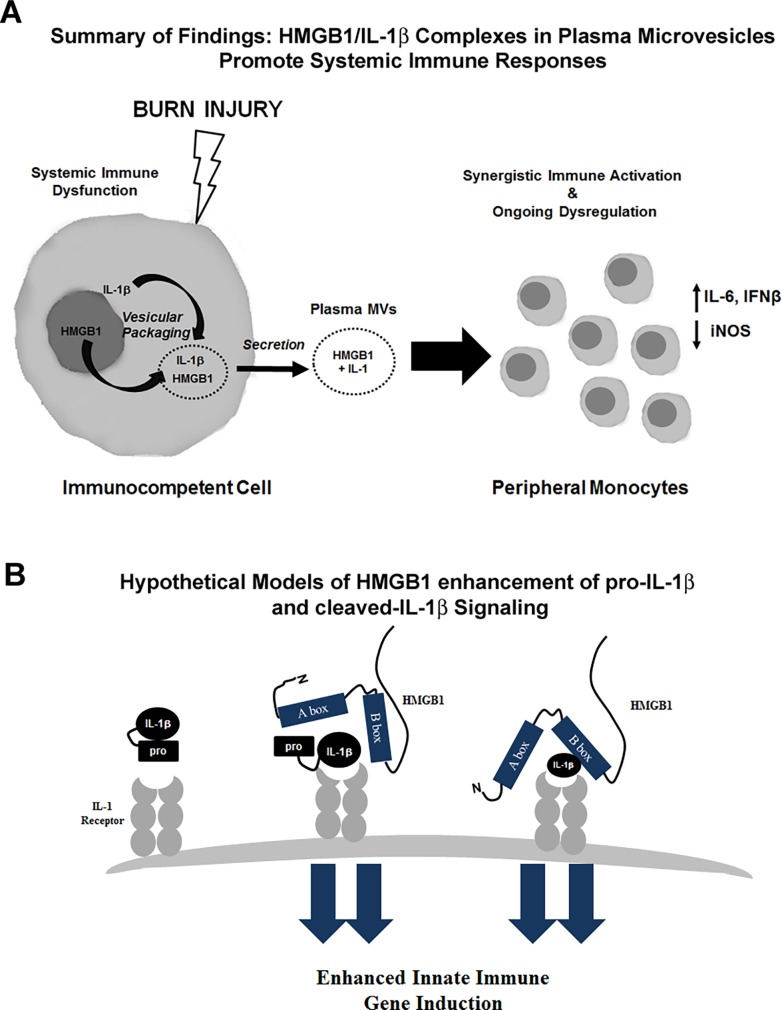
Modulating immune responses to sepsis and trauma remain one of the most difficult challenges in modern medicine. Large burn injuries (LBI) are a severe form of trauma associated with sepsis, immune impairment, and mortality. Immune dysfunction after LBI is complex, involving both enhanced and impaired immune activation. The release of Damage-Associated Molecular Patterns (DAMPs), such as HMGB1, and cytokines (e.g. IL-1β) creates an environment of immune dysfunction often leading to end organ failure and death. Both HMGB1 and IL-1β have been found to play critical roles in sepsis and post-burn immune dysfunction. HMGB1 and IL-1β have been shown previously to form potent complexes in vitro. We recently identified the presence of HMGB1/IL-1β heterocomplexes in human tissue. We now find HMGB1/IL-1β complexes in human and mouse plasma, and identify a synergistic role of HMGB1/IL-1β complexes in post-burn immune dysfunction. In both humans and mice, we found that HMGB1 was enriched in plasma microvesicles (MVs) after LBI. HMGB1 was found form complexes with IL-1β. Using flow cytometry of mouse plasma MVs, we identified an increase in an HMGB1+/IL-1β+ MVs. Using co-IP, HMGB1 was found to bind the pro-form of IL-1β in mouse and human plasma. Pro-IL-1β, which is traditionally considered inactive, became active when complexed with HMGB1. Human THP-1 monocytes treated with HMGB1-pro-IL-1β complexes showed increased transcription of LBI associated cytokines IL-6 and IFNβ along with suppression of iNOS, mimicking findings associated with LBI. These findings identify that HMGB1/IL-1β complexes released after burn injuries can modulate immune responses, and microvesicles are identified as a novel reservoir for these immune mediators. These complexes might serve as novel immune targets for the treatment of systemic immune responses due to LBI or other causes of sepsis.
Conflict of interest statement
Figures
References
-
- Yang H, Ochani M, Li J, Qiang X, Tanovic M, Harris HE, et al. Reversing established sepsis with antagonists of endogenous high-mobility group box 1. Proceedings of the National Academy of Sciences of the United States of America. 2004;101(1):296–301. doi: 10.1073/pnas.2434651100 ; PubMed Central PMCID: PMC314179. - DOI - PMC - PubMed
-
- Lamkanfi M, Sarkar A, Vande Walle L, Vitari AC, Amer AO, Wewers MD, et al. Inflammasome-dependent release of the alarmin HMGB1 in endotoxemia. Journal of immunology. 2010;185(7):4385–92. doi: 10.4049/jimmunol.1000803 ; PubMed Central PMCID: PMCPMC3428148. - DOI - PMC - PubMed
-
- Wang H, Bloom O, Zhang M, Vishnubhakat JM, Ombrellino M, Che J, et al. HMG-1 as a late mediator of endotoxin lethality in mice. Science. 1999;285(5425):248–51. . - PubMed
-
- Opal SM, Fisher CJ Jr., Dhainaut JF, Vincent JL, Brase R, Lowry SF, et al. Confirmatory interleukin-1 receptor antagonist trial in severe sepsis: a phase III, randomized, double-blind, placebo-controlled, multicenter trial. The Interleukin-1 Receptor Antagonist Sepsis Investigator Group. Critical care medicine. 1997;25(7):1115–24. . - PubMed
-
- Fisher CJ Jr., Dhainaut JF, Opal SM, Pribble JP, Balk RA, Slotman GJ, et al. Recombinant human interleukin 1 receptor antagonist in the treatment of patients with sepsis syndrome. Results from a randomized, double-blind, placebo-controlled trial. Phase III rhIL-1ra Sepsis Syndrome Study Group. JAMA. 1994;271(23):1836–43. . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
