

Efficacy and Safety of Tadalafil 5 mg Once Daily for the Treatment of Erectile Dysfunction After Robot-Assisted Laparoscopic Radical Prostatectomy: A 2-Year Follow-Up
- PMID: 29602721
- PMCID: PMC5960019
- DOI: 10.1016/j.esxm.2017.12.005
Efficacy and Safety of Tadalafil 5 mg Once Daily for the Treatment of Erectile Dysfunction After Robot-Assisted Laparoscopic Radical Prostatectomy: A 2-Year Follow-Up
Erratum in
-
Erratum.Sex Med. 2018 Sep;6(3):272. doi: 10.1016/j.esxm.2018.06.001. Epub 2018 Jul 27. Sex Med. 2018. PMID: 30061061 Free PMC article. No abstract available.
Abstract
Background: Although nerve-sparing robot-assisted radical prostatectomy (NS-RALP) is performed, a large number of patients still experience erectile dysfunction (ED) after surgery.
Aim: To evaluate the efficacy and safety of tadalafil 5 mg once daily (OaD) in ED treatment over 2 years and investigate the cause of vascular ED after NS-RARP.
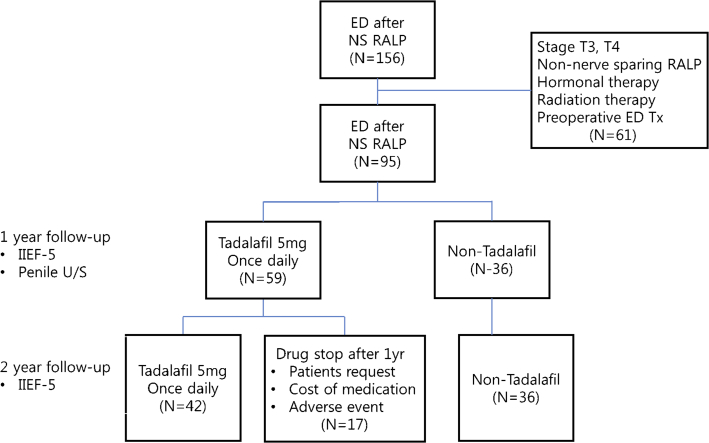
Methods: We retrospectively evaluated 95 men who underwent NS-RARP and had a penile rehabilitation treatment with tadalafil 5 mg OaD. They were classified into 3 groups: tadalafil 5 mg OaD for 2 years (group I), tadalafil 5 mg OaD for 1 year (group II), and no tadalafil (group III). All patients in group I underwent penile color duplex ultrasound to evaluate the cause of vascular ED.
Outcomes: Patients were surveyed using the abridged 5-item International Index of Erectile Function (IIEF-5).
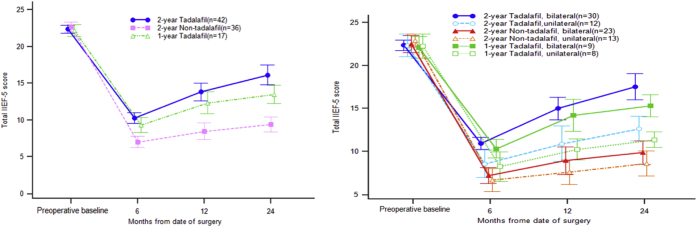
Results: Statistically significant improvements were observed in group I for all IIEF-5 domain scores (P = .000). There was no statistically significant difference in recovery of erectile function (EF) the 2-year follow-up between groups I and II. Sub-analysis based on NS status showed no difference in recovery of EF. However, group I showed better trends in EF improvement. Those with venogenic ED had poor responses compared with those with arteriogenic ED or unremarkable findings with tadalafil 5-mg OaD treatment (14.2% vs 55.0% vs 53.3%). The overall side effects included hot flushing in 9.5%, headache in 7.1%, and dizziness in 2.3% of patients.
Clinical implications: Long-term usage of tadalafil 5 mg OaD after RARP can be an effective option for penile rehabilitation.
Strengths and limitations: The present study is a retrospective study with a relatively small sample.
Conclusions: Although the responses of patients with venogenic ED were limited compared with those with arteriogenic ED, tadalafil 5-mg OaD treatment was well tolerated and significantly improved EF up to 2 years after NS-RARP. Kim S, Sung GT. Efficacy and Safety of Tadalafil 5 mg Once Daily for the Treatment of Erectile Dysfunction After Robot-Assisted Laparoscopic Radical Prostatectomy: A 2-Year Follow-Up. Sex Med 2018;6:108-114.
Keywords: Erectile Dysfunction; Penile Rehabilitation; Phosphodiesterase Type 5 Inhibitor; Robot-Assisted Radical Prostatectomy.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Re: Efficacy and Safety of Tadalafil 5 mg Once Daily for the Treatment of Erectile Dysfunction after Robot-Assisted Laparoscopic Radical Prostatectomy: A 2-Year Follow-up.J Urol. 2018 Sep;200(3):481. doi: 10.1016/j.juro.2018.05.112. Epub 2018 May 30. J Urol. 2018. PMID: 30412950 No abstract available.
References
-
- Heidenreich A., Bastian P.J., Bellmunt J. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol. 2014;65:124–137. - PubMed
-
- Zippe C.D., Pahlajani G. Penile rehabilitation following radical prostatectomy: role of early intervention and chronic therapy. Urol Clin North Am. 2007;34:601–618. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
