

Does Enhancement or Perfusion on Preprocedure CT Predict Outcomes After Embolization of Hepatocellular Carcinoma?
- PMID: 29602726
- PMCID: PMC6160360
- DOI: 10.1016/j.acra.2018.02.027
Does Enhancement or Perfusion on Preprocedure CT Predict Outcomes After Embolization of Hepatocellular Carcinoma?
Abstract
Rationale and objective: The objective of this study was to evaluate whether quantitative enhancement or perfusion measurements on preprocedure triphasic computed tomography (CT) can be used to predict response or overall survival after embolization of hepatocellular carcinoma.
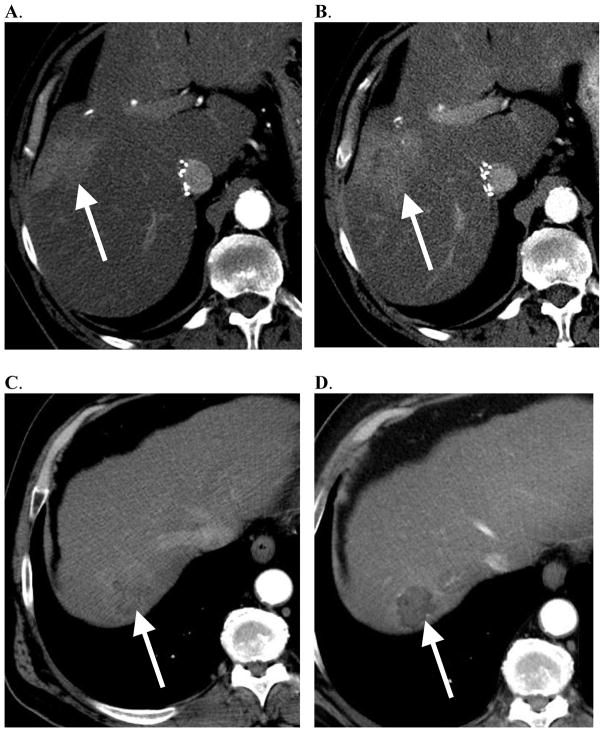
Materials and methods: The institutional review board approved this retrospective review of 63 patients with hepatocellular carcinoma treated with particle embolization between March 2009 and December 2014. Quantitative enhancement and perfusion measurements were performed on the target tumor and the background liver on the triphasic CT performed before treatment. Microvascular invasion (MVI) and degree of differentiation were determined from a core biopsy specimen. Quantitative enhancement and perfusion values were then correlated with pathology (two-tailed t test), response to embolization on modified Response Evaluation Criteria In Solid Tumors (two-tailed t test), and overall survival after embolization (Cox proportional hazards model).
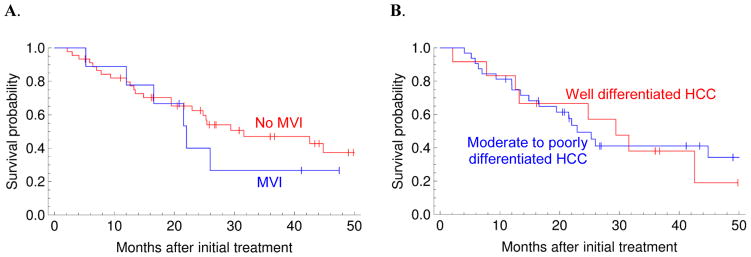
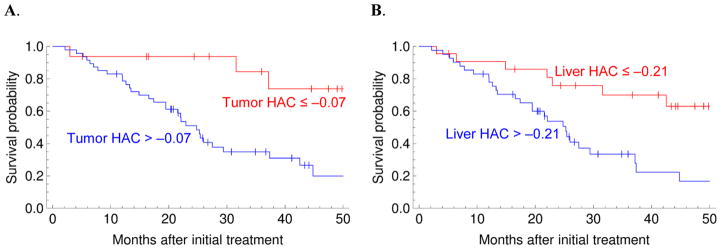
Results: Arterial enhancement did not predict immediate response or overall survival after embolization. The degree of differentiation or presence of MVI also did not predict immediate response or overall survival after embolization. However, high hepatic artery coefficient or low portal vein coefficient, both in the tumor (P = .011 and P = .004) and in the background liver (P = .015 and P = .009), were associated with worse survival. Hepatic artery coefficient, both in the tumor (P = .025) and in the background liver (P = .013), were independent predictors of survival in a multivariate model including the Child-Pugh score and the BCLC stage.
Conclusions: Tumor and liver perfusion parameters estimated from preprocedure triphasic CT were predictive of survival after embolization. Arterial-phase enhancement and histology (degree of differentiation or MVI) did not predict immediate response or overall survival after particle embolization.
Keywords: Hepatocellular carcinoma; blood supply; cirrhosis; hypovascular; perfusion.
Copyright © 2018 The Association of University Radiologists. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Vilgrain V, Bouattour M, Sibert A, et al. SARAH: A randomised controlled trial comparing efficacy and safety of selective internal radiation therapy (with yttrium-90 microspheres) and sorafenib in patients with locally advanced hepatocellular carcinoma. Journal of Hepatology. 2017;66(1, Supplement):S85–6.
-
- Biederman DM, Titano JJ, Tabori NE, et al. Outcomes of Radioembolization in the Treatment of Hepatocellular Carcinoma with Portal Vein Invasion: Resin versus Glass Microspheres. J Vasc Interv Radiol. 2016;27(6):812–21e2. - PubMed
-
- Katyal S, Oliver JH, Peterson MS, Chang PJ, Baron RL, Carr BI. Prognostic significance of arterial phase CT for prediction of response to transcatheter arterial chemoembolization in unresectable hepatocellular carcinoma: a retrospective analysis. AJR Am J Roentgenol. 2000;175(6):1665–72. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
