

An in vivo analysis of safe laparoscopic grasping thresholds for colorectal surgery
- PMID: 29602989
- PMCID: PMC6132882
- DOI: 10.1007/s00464-018-6172-6
An in vivo analysis of safe laparoscopic grasping thresholds for colorectal surgery
Abstract
Background: Analysis of safe laparoscopic grasping thresholds for the colon has not been performed. This study aimed to analyse tissue damage thresholds when the colon is grasped laparoscopically, correlating histological changes to mechanical compressive forces.
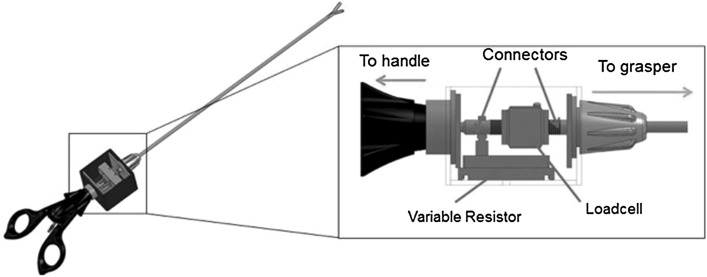
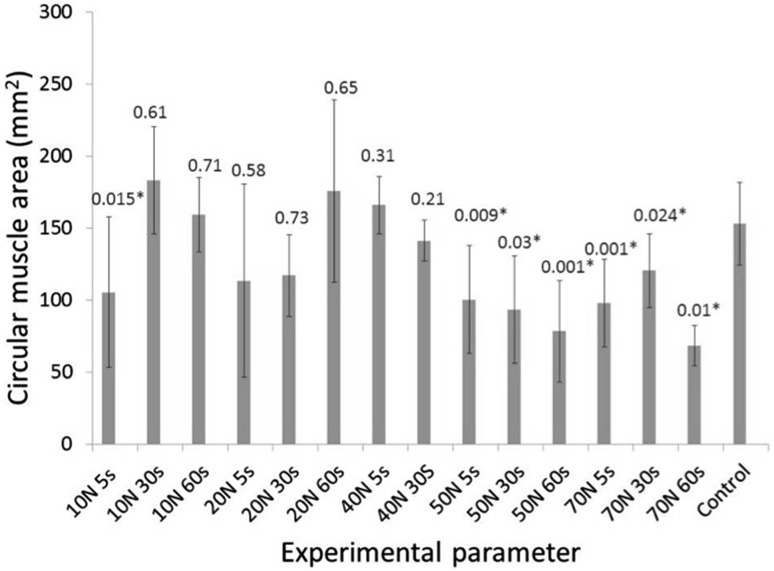
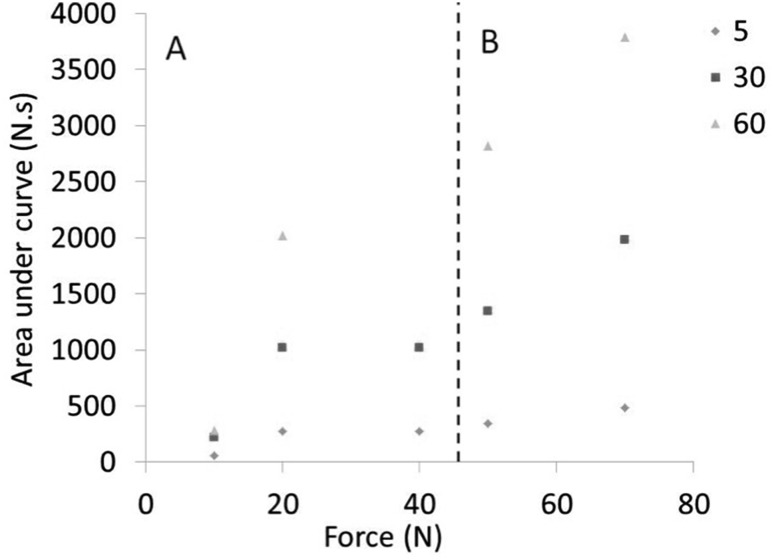
Methods: An instrumented laparoscopic grasper was used to measure the forces applied to porcine colon, with data captured and plotted as a force-time (f-t) curve. Haematoxylin and eosin histochemistry of tissue subjected to 10, 20, 40, 50 and 70 N for 5, 30 and 60 s was performed, and the area of colonic circular and longitudinal muscle was compared in grasped and un-grasped regions. The area under the f-t curve was calculated as a measure of the accumulated force applied, known as the force-time product (FTP).
Results: FTP ranged from 55.7 to 3793 N.s. Significant differences were observed between the muscle area of the grasped and un-grasped regions in both longitudinal and circular muscle at 50 N and above for all grasping times. For the longitudinal muscle, significant differences were observed between grasped and un-grasped areas at 20 N force for 30 s (mean difference = 59 mm2, 95% CI 41-77 mm2, P = 0.04), 20 N force for 60 s (mean difference = 31 mm2, 95% CI 21.5-40.5 mm2, P = 0.006) and 40 N force for 30 s (mean difference 37 mm2, 95% CI 27-47 mm2, P = 0.006). Changes in histology correlated with mechanical forces applied to the longitudinal muscle at a FTP over 300 N s.
Conclusions: This study characterizes the grasping forces that result in histological changes to the colon and correlates these with a mechanical measurement of the applied force. The findings will contribute to the development of smart laparoscopic graspers with active constraints to prevent excessive grasping and tissue injury.
Keywords: Colon; Grasping; Laparoscopy.
Conflict of interest statement
The authors Miss Jenifer Barrie, Dr Louise Russell, Mr Adrian Hood, Professor Anne Neville, Professor David Jayne and Dr Peter Culmer have no conflicts of interest or financial ties to disclose.
Figures



References
-
- Barrie J, Jayne DG, Neville A, Hunter L, Hood AJ, Culmer PR. Real-time measurement of the tool-tissue interaction in minimally invasive abdominal surgery the first step to developing the next generation of smart laparoscopic instruments. Surg Innov. 2016;23:463–468. doi: 10.1177/1553350616646475. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
