

Fetal Intelligent Navigation Echocardiography (FINE) Detects 98% of Congenital Heart Disease
- PMID: 29603310
- PMCID: PMC6165712
- DOI: 10.1002/jum.14616
Fetal Intelligent Navigation Echocardiography (FINE) Detects 98% of Congenital Heart Disease
Abstract
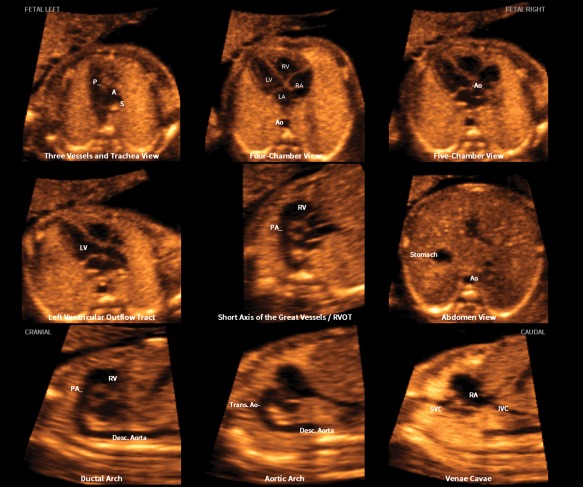
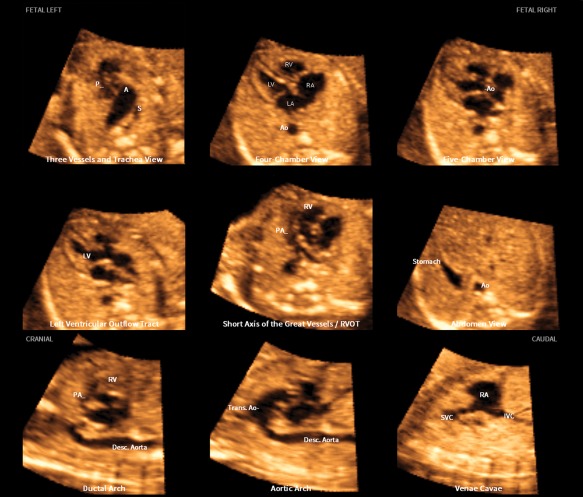
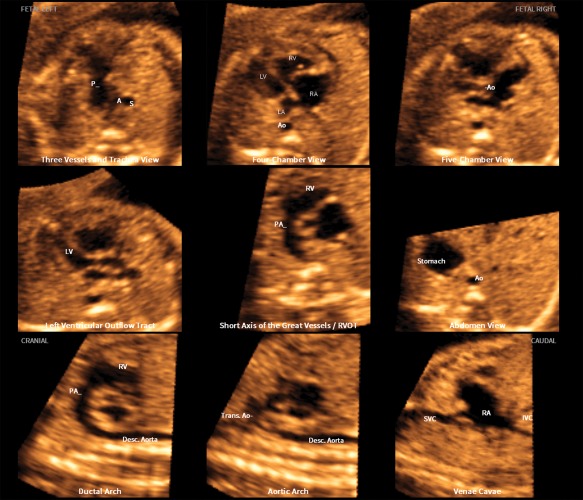
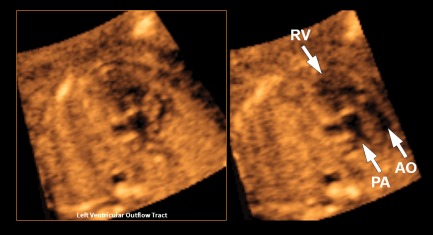
Objective: Fetal intelligent navigation echocardiography (FINE) is a novel method that automatically generates and displays 9 standard fetal echocardiographic views in normal hearts by applying intelligent navigation technology to spatiotemporal image correlation (STIC) volume data sets. The main objective was to determine the sensitivity and specificity of FINE in the prenatal detection of congenital heart disease (CHD).
Methods: A case-control study was conducted in 50 fetuses with a broad spectrum of CHD (cases) and 100 fetuses with normal hearts (controls) in the second and third trimesters. Using 4-dimensional ultrasound with STIC technology, volume data sets were acquired. After all identifying information was removed, the data sets were randomly distributed to a different investigator for analysis using FINE. The sensitivity and specificity for the prenatal detection of CHD, as well as positive and negative likelihood ratios were determined.
Results: The diagnostic performance of FINE for the prenatal detection of CHD was: sensitivity of 98% (49 of 50), specificity of 93% (93 of 100), positive likelihood ratio of 14, and negative likelihood ratio of 0.02. Among cases with confirmed CHD, the diagnosis with use of FINE completely matched the final diagnosis in 74% (37 of 50); minor discrepancies were seen in 12% (6 of 50), and major discrepancies were seen in 14% (7 of 50).
Conclusions: This is the first time the sensitivity and specificity of the FINE method in fetuses with normal hearts and CHD in the second and third trimesters has been reported. Because FINE identifies a broad spectrum of CHD with 98% sensitivity, this method could be used prenatally to screen for and diagnose CHD.
Keywords: 4-dimensional; cardiac; fetal heart; prenatal diagnosis; spatiotemporal image correlation; ultrasound.
© 2018 The Authors. Journal of Ultrasound in Medicine published by the American Institute of Ultrasound in Medicine.
Figures
Similar articles
-
New and advanced features of fetal intelligent navigation echocardiography (FINE) or 5D heart.J Matern Fetal Neonatal Med. 2022 Apr;35(8):1498-1516. doi: 10.1080/14767058.2020.1759538. Epub 2020 May 6. J Matern Fetal Neonatal Med. 2022. PMID: 32375528 Free PMC article.
-
Color and power Doppler combined with Fetal Intelligent Navigation Echocardiography (FINE) to evaluate the fetal heart.Ultrasound Obstet Gynecol. 2017 Oct;50(4):476-491. doi: 10.1002/uog.17522. Epub 2017 Aug 14. Ultrasound Obstet Gynecol. 2017. PMID: 28809063 Free PMC article.
-
Fetal Intelligent Navigation Echocardiography (FINE): a novel method for rapid, simple, and automatic examination of the fetal heart.Ultrasound Obstet Gynecol. 2013 Sep;42(3):268-84. doi: 10.1002/uog.12563. Ultrasound Obstet Gynecol. 2013. PMID: 24000158 Free PMC article.
-
Prenatal Diagnosis of Dextrocardia with Complex Congenital Heart Disease Using Fetal Intelligent Navigation Echocardiography (FINE) and a Literature Review.Fetal Diagn Ther. 2018;43(4):304-316. doi: 10.1159/000468929. Epub 2017 Jun 23. Fetal Diagn Ther. 2018. PMID: 28641300 Free PMC article. Review.
-
Contemporary clinical applications of spatio-temporal image correlation in prenatal diagnosis.Curr Opin Obstet Gynecol. 2011 Apr;23(2):94-102. doi: 10.1097/GCO.0b013e328342ef38. Curr Opin Obstet Gynecol. 2011. PMID: 21178772 Review.
Cited by
-
Semi-Automatic Measurement of Fetal Cardiac Axis in Fetuses with Congenital Heart Disease (CHD) with Fetal Intelligent Navigation Echocardiography (FINE).J Clin Med. 2023 Oct 5;12(19):6371. doi: 10.3390/jcm12196371. J Clin Med. 2023. PMID: 37835015 Free PMC article.
-
Application of Semiautomatic Fetal Intelligent Navigation Echocardiography (FINE) in Twin Pregnancies: Half the Work or Twice the Effort?Cureus. 2023 Apr 24;15(4):e38052. doi: 10.7759/cureus.38052. eCollection 2023 Apr. Cureus. 2023. PMID: 37228519 Free PMC article.
-
A deep-learning pipeline to diagnose pediatric intussusception and assess severity during ultrasound scanning: a multicenter retrospective-prospective study.NPJ Digit Med. 2023 Sep 30;6(1):182. doi: 10.1038/s41746-023-00930-8. NPJ Digit Med. 2023. PMID: 37775624 Free PMC article.
-
Prenatal Diagnosis and Fetopsy Validation of Complete Atrioventricular Septal Defects Using the Fetal Intelligent Navigation Echocardiography Method.Diagnostics (Basel). 2023 Jan 26;13(3):456. doi: 10.3390/diagnostics13030456. Diagnostics (Basel). 2023. PMID: 36766561 Free PMC article.
-
New and advanced features of fetal intelligent navigation echocardiography (FINE) or 5D heart.J Matern Fetal Neonatal Med. 2022 Apr;35(8):1498-1516. doi: 10.1080/14767058.2020.1759538. Epub 2020 May 6. J Matern Fetal Neonatal Med. 2022. PMID: 32375528 Free PMC article.
References
-
- Simeone RM, Feldkamp ML, Reefhuis J, et al. CDC Grand Rounds: understanding the causes of major birth defects: steps to prevention. MMWR Morb Mortal Wkly Rep 2015; 64:1104–1107. - PubMed
-
- Yang Q, Chen H, Correa A, Devine O, Mathews TJ, Honein MA. Racial differences in infant mortality attributable to birth defects in the United States, 1989–2002. Birth Defects Res A Clin Mol Teratol 2006; 76:706–713. - PubMed
-
- Friedberg MK, Silverman NH, Moon‐Grady AJ, et al. Prenatal detection of congenital heart disease. J Pediatr 2009; 155:26–31. - PubMed
-
- Jaeggi ET, Sholler GF, Jones OD, Cooper SG. Comparative analysis of pattern, management and outcome of pre‐ versus postnatally diagnosed major congenital heart disease: a population‐based study. Ultrasound Obstet Gynecol 2001; 17:380–385. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
