

Natural history of myocardial deformation in children, adolescents, and young adults exposed to anthracyclines: Systematic review and meta-analysis
- PMID: 29603386
- PMCID: PMC6544758
- DOI: 10.1111/echo.13871
Natural history of myocardial deformation in children, adolescents, and young adults exposed to anthracyclines: Systematic review and meta-analysis
Abstract
Objective: Anthracyclines are widely used to treat solid and hematologic malignancies, but are known to cause cardiotoxicity. As more childhood cancer survivors reach adulthood due to improvements in oncologic treatments, they become susceptible to late and progressive anthracycline-induced cardiotoxicity. Nonetheless, diagnostic criteria for early detection of cardiac dysfunction are not well defined in children, adolescent, and young adults (CAYA, ages 1-40 years). We present a natural history of the changes in myocardial deformation in CAYA patients after anthracycline therapy.
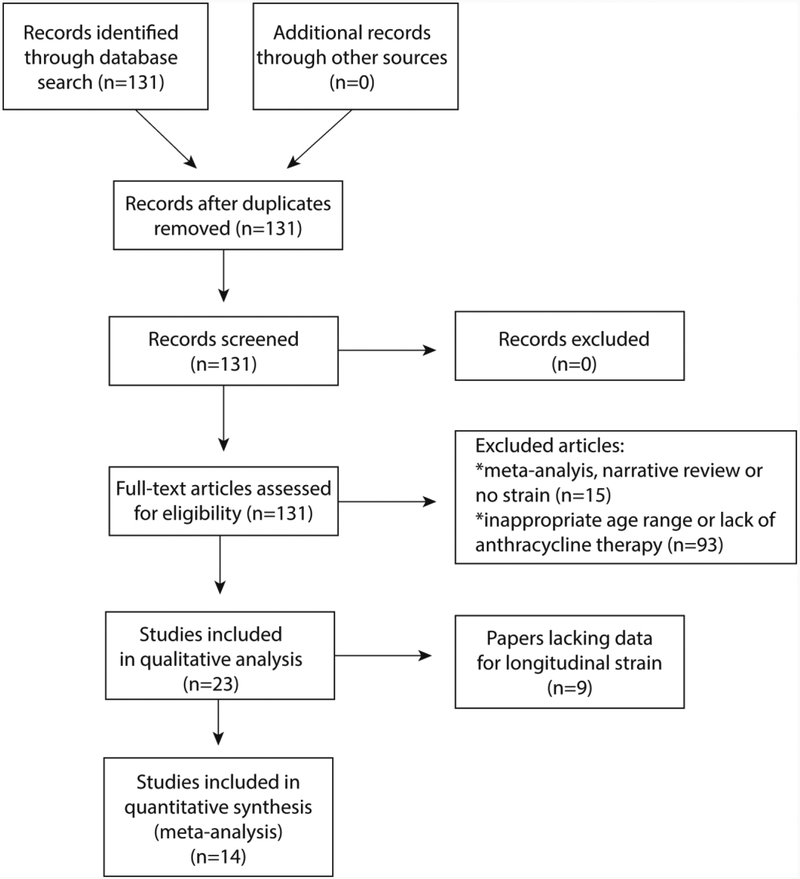
Methods: We performed a literature review search between 2001 and 2016 using PubMed with the following search terms: strain (or deformation), torsion (or twist), children (or adolescent or young adult), cardiotoxicity (or dysfunction), and anthracyclines (or doxorubicin). A total of 23 articles were reviewed. Fourteen articles were incorporated in the meta-analysis.
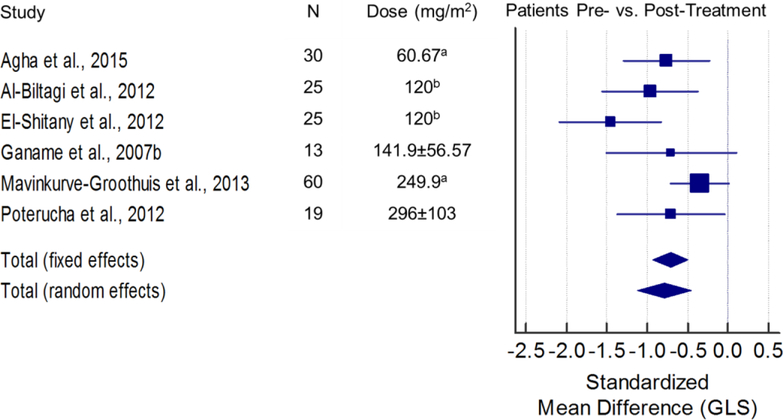
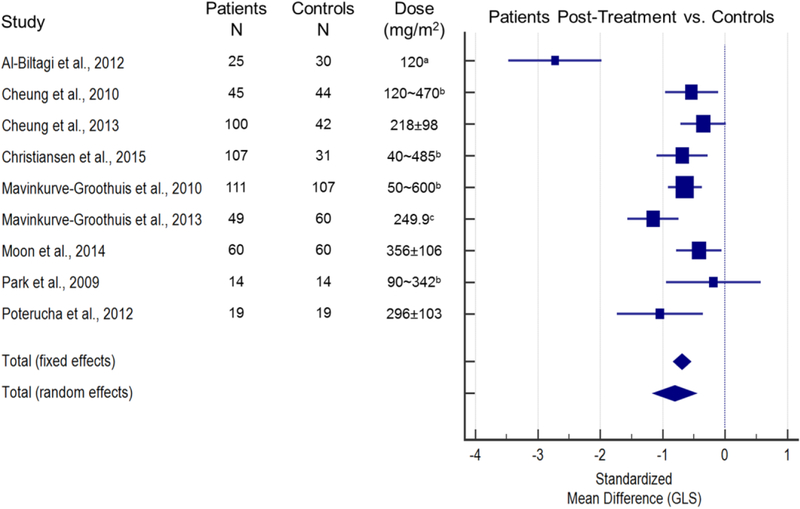
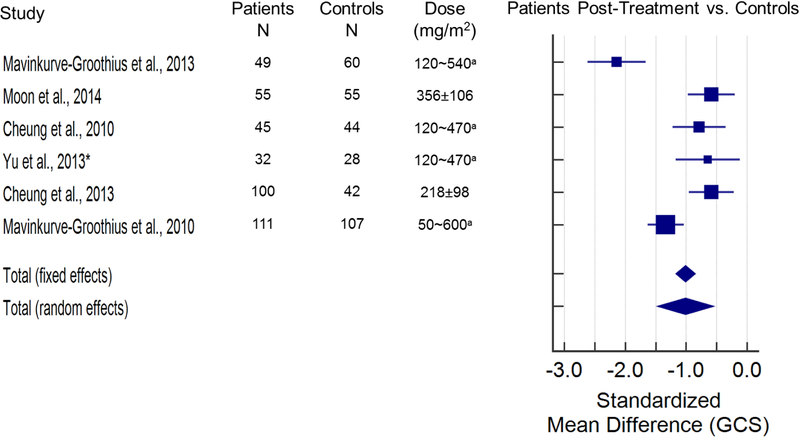
Results: Strain abnormalities are observed at both short-term and long-term follow-up. Global longitudinal strain (GLS) abnormalities are common during or early after chemotherapy, whereas changes in global circumferential strain (GCS) are more significant and consistent on long-term follow-up. Although global radial strain and torsional parameters are also often abnormal late after chemotherapy, there are few studies evaluating these parameters.
Conclusion: There are significant abnormalities in GLS and GCS following anthracycline therapy acutely and late after treatment. The prognostic value of these strain abnormalities warrants further investigation.
Keywords: cardiac toxicity; myocardial strain; transthoracic echocardiography.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
Figures
References
-
- Lipshultz SE, Cochran TR, Franco VI MT. Treatment-related cardiotoxicity in survivors of childhood cancer. Nat Rev Clin Oncol. 2013;10:697–710. - PubMed
-
- Bijnens B, Cikes M, Butakoff C, Sitges M CF. Myocardial motion and deformation: What does it tell us and how does it relate to function? Fetal Diagn Ther. 2012;32:5–16. - PubMed
-
- Di Marco A, Cassinelli G AF. The discovery of daunorubicin. Cancer Treat Rep. 1981;65:3–8. - PubMed
-
- Reulen RC, Winter DL, Frobisher C, Lancashire ER, Stiller CA, Jenney ME, Skinner R, Stevens MC HMBCCSSSG. Long-term cause-specific mortality among survivors of childhood cancer. JAMA. 2010;304:172–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
