

Time trends in service provision and survival outcomes for patients with renal cancer treated by nephrectomy in England 2000-2010
- PMID: 29603575
- PMCID: PMC6175431
- DOI: 10.1111/bju.14217
Time trends in service provision and survival outcomes for patients with renal cancer treated by nephrectomy in England 2000-2010
Abstract
Objective: To describe the temporal trends in nephrectomy practice and outcomes for English patients with renal cell carcinoma (RCC).
Patients and methods: Adult RCC nephrectomy patients treated between 2000 and 2010 were identified in the National Cancer Data Repository and Hospital Episode Statistics, and followed-up until date of death or 31 December 2015 (n = 30 763). We estimated the annual frequency for each nephrectomy type, the hospital and surgeon numbers and their case volumes. We analysed short-term surgical outcomes, as well as 1- and 5-year relative survivals.
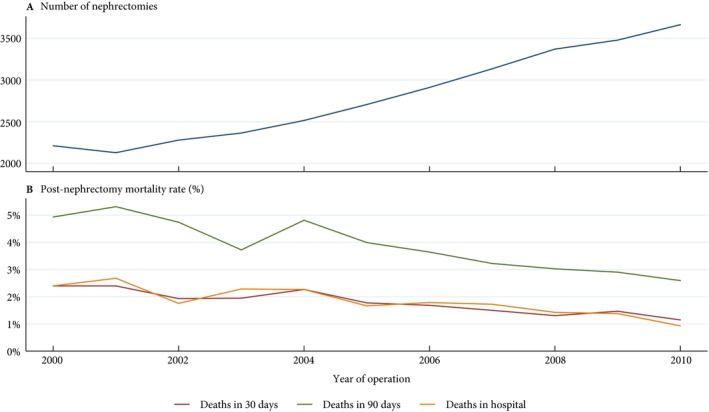
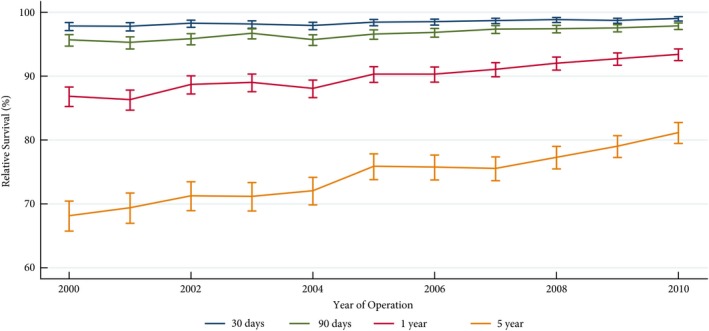
Results: Annual RCC nephrectomy number increased by 66% during the study period. Hospital number decreased by 24%, whilst the median annual hospital volume increased from 10 to 23 (P < 0.01). Surgeon number increased by 27% (P < 0.01), doubling the median consultant number per hospital. The proportion of minimally invasive surgery (MIS) nephrectomies rose from 1% to 46%, whilst the proportion of nephron-sparing surgeries (NSS) increased from 5% to 16%, with 29% of all T1 disease treated with partial nephrectomy in 2010 (P < 0.01). The 30-day mortality rate halved from 2.4% to 1.1% and 90-day mortality decreased from 4.9% to 2.6% (P < 0.01). The 1-year relative survival rate increased from 86.9% to 93.4%, whilst the 5-year relative survival rate rose from 68.2% to 81.2% (P < 0.01). Improvements were most notable in patients aged ≥65 years and those with T3 and T4 disease.
Conclusions: Surgical RCC management has changed considerably with nephrectomy centralisation and increased NSS and MIS. In parallel, we observed significant improvements in short- and long-term survival particularly for elderly patients and those with locally advanced disease.
Keywords: #KidneyCancer; centralisation; nephrectomy; postoperative outcomes; renal cancer; survival.
© 2018 The Authors BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Figures
Comment in
-
Re: Time Trends in Service Provision and Survival Outcomes for Patients with Renal Cancer Treated by Nephrectomy in England 2000-2010.J Urol. 2019 May;201(5):855. doi: 10.1097/JU.0000000000000167. J Urol. 2019. PMID: 30747866 No abstract available.
Similar articles
-
Evolving trends in the surgical management of renal masses over the past two decades: A contemporary picture from a large prospectively-maintained database.Int J Urol. 2019 Apr;26(4):465-474. doi: 10.1111/iju.13909. Epub 2019 Feb 28. Int J Urol. 2019. PMID: 30818418
-
Variation in use of nephron-sparing surgery among children with renal tumors.J Pediatr Urol. 2014 Aug;10(4):724-9. doi: 10.1016/j.jpurol.2013.12.019. Epub 2014 Jan 22. J Pediatr Urol. 2014. PMID: 24517904 Free PMC article.
-
Age distribution for partial and radical nephrectomy: whose nephrons are being spared?Adv Ther. 2013 Oct;30(10):924-32. doi: 10.1007/s12325-013-0061-0. Epub 2013 Oct 24. Adv Ther. 2013. PMID: 24155056
-
Laparoscopic and partial nephrectomy.Clin Cancer Res. 2004 Sep 15;10(18 Pt 2):6322S-7S. doi: 10.1158/1078-0432.CCR-050003. Clin Cancer Res. 2004. PMID: 15448025 Review.
-
[Positive surgical margins in nephron sparing surgery for renal cell carcinoma].Urologia. 2014 Jan-Mar;81(1):30-9. doi: 10.5301/uro.5000067. Urologia. 2014. PMID: 24803357 Review. Italian.
Cited by
-
Personalized Prediction of Long-Term Renal Function Prognosis Following Nephrectomy Using Interpretable Machine Learning Algorithms: Case-Control Study.JMIR Med Inform. 2024 Sep 20;12:e52837. doi: 10.2196/52837. JMIR Med Inform. 2024. PMID: 39303280 Free PMC article.
-
Surgical Trends and Complications in Partial and Radical Nephrectomy: Results from the GRAND Study.Cancers (Basel). 2023 Dec 24;16(1):97. doi: 10.3390/cancers16010097. Cancers (Basel). 2023. PMID: 38201523 Free PMC article.
-
The roles of ferroptosis regulatory gene SLC7A11 in renal cell carcinoma: A multi-omics study.Cancer Med. 2021 Dec;10(24):9078-9096. doi: 10.1002/cam4.4395. Epub 2021 Nov 10. Cancer Med. 2021. PMID: 34761566 Free PMC article.
-
Impact of hospital nephrectomy volume on intermediate- to long-term survival in renal cell carcinoma.BJU Int. 2020 Jan;125(1):56-63. doi: 10.1111/bju.14848. Epub 2019 Jul 15. BJU Int. 2020. PMID: 31206987 Free PMC article.
-
Comparing Long-Term Outcomes Following Radical and Partial Nephrectomy for cT1 Renal Cell Carcinoma in Young and Healthy Individuals.JNCI Cancer Spectr. 2019 Feb 1;3(1):pkz003. doi: 10.1093/jncics/pkz003. eCollection 2019 Mar. JNCI Cancer Spectr. 2019. Retraction in: JNCI Cancer Spectr. 2020 Oct 17;4(4):pkaa056. doi: 10.1093/jncics/pkaa056. PMID: 31360891 Free PMC article. Retracted.
References
-
- Znaor A, Lortet‐Tieulent J, Laversanne M, Jemal A, Bray F. International variations and trends in renal cell carcinoma incidence and mortality. Eur Urol 2015; 67: 519–30 - PubMed
-
- Cancer Research UK . Kidney Cancer Incidence Statistics, 2016. Available at: http://www.cancerresearchuk.org. Accessed April 2017.
-
- De Angelis R, Sant M, Coleman MP et al. Cancer survival in Europe 1999‐2007 by country and age: results of EUROCARE‐5‐a population‐based study. Lancet Oncol 2014; 15: 23–34 - PubMed
-
- Sant M, Allemani C, Santaquilani M et al. EUROCARE‐4. Survival of cancer patients diagnosed in 1995‐1999. Results and commentary. Eur J Cancer 2009; 45: 931–91 - PubMed
-
- National Institute for Clinical Excellence . Improving outcomes in urological cancers. Cancer service guideline [CSG2], 2002. Available at: https://www.nice.org.uk/guidance/csg2. Accessed March 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
