

Treatment trends and Medicare reimbursements for localized prostate cancer in elderly patients
- PMID: 29603911
- PMCID: PMC6118049
- DOI: 10.5489/cuaj.4865
Treatment trends and Medicare reimbursements for localized prostate cancer in elderly patients
Abstract
Introduction: The absolute and proportional numbers of elderly patients diagnosed with localized prostate cancer (PCa) are on the rise. We examined treatment trends and reimbursement figures in localized PCa patients aged ≥80 years.
Methods: Between 2000 and 2008, we identified 30 217 localized PCa patients aged ≥80 years in Surveillance, Epidemiology, and End Results (SEER)-Medicare-linked database. Alternative treatment modalities consisted of conservative management (CM), radiation therapy (RT), radical prostatectomy (RP), and primary androgen-deprivation therapy (PADT). For all four modalities, utilization and reimbursements were examined.
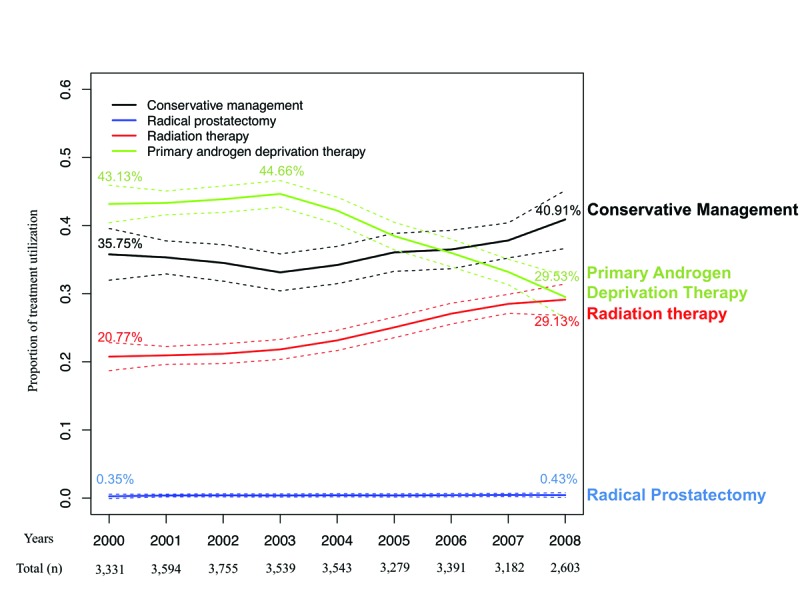
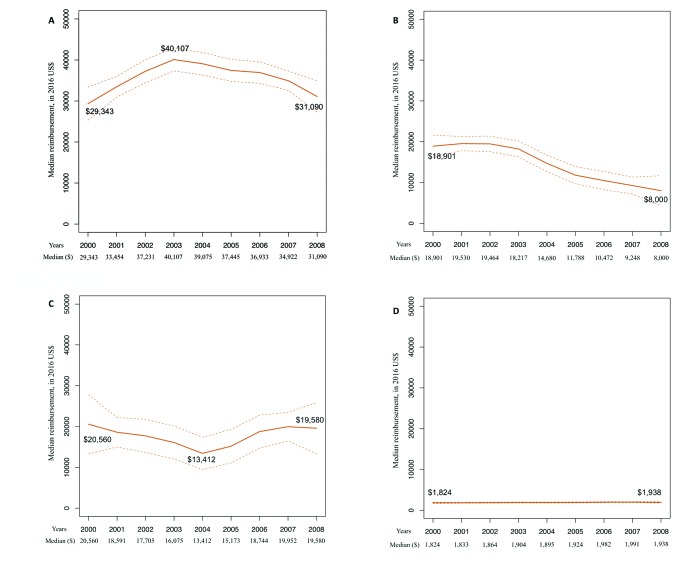
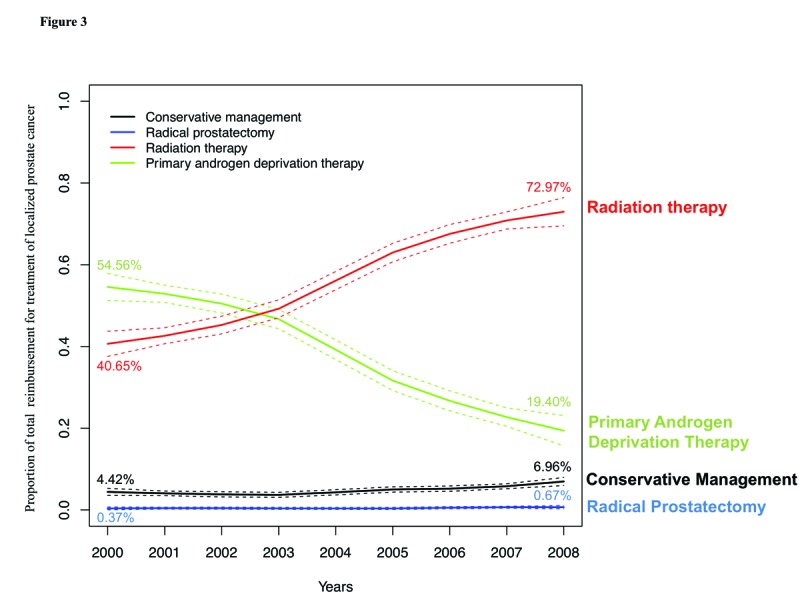
Results: PADT was the most frequently used treatment modality between 2000 and 2005. CM became the dominant treatment modality from 2006-2008. RP rates were marginal. RT ranked third, and its annual rate increased from 20.77% in 2000 to 29.13% in 2008. Median individual reimbursement of RT was highest and ranged from $29 343 in 2000 to $31 090 in 2008, followed by RP (from $20 560 in 2000 to $19 580 in 2008), PADT (from $18 901 in 2000 to $8000 in 2008), and CM (from $1824 in 2000 to $1938 in 2008). RT contributed to most of the cumulative annual reimbursements from 2003 (49.24%) to 2008 (72.97%). PADT ranked first from 2000 (54.56%) to 2002 (50.49%), but decreased by 19.40% in 2008. CM's contribution increased from 4.42% in 2000 to 6.96% in 2008. RP's share of reimbursements was stable during the study period.
Conclusions: Our results, focusing on localized PCa treatment in patients aged ≥80 years, showed an important increase in rates, median cost, and proportion of cumulative cost related to RT.
Conflict of interest statement
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975–2012. National Cancer Institute; [Accessed June 7, 2018]. [Updated Nov. 18, 2015]. Avaialble at https://seer.cancer.gov/archive/csr/1975_2012/
-
- Guidelines on prostate cancer. European Association of Urology; 2017. [Accessed June 7, 2018]. Available at http://uroweb.org/guideline/prostate-cancer/
LinkOut - more resources
Full Text Sources
Other Literature Sources
