

Developing and validating a new precise risk-prediction model for new-onset hypertension: The Jichi Genki hypertension prediction model (JG model)
- PMID: 29604170
- PMCID: PMC8031110
- DOI: 10.1111/jch.13270
Developing and validating a new precise risk-prediction model for new-onset hypertension: The Jichi Genki hypertension prediction model (JG model)
Abstract
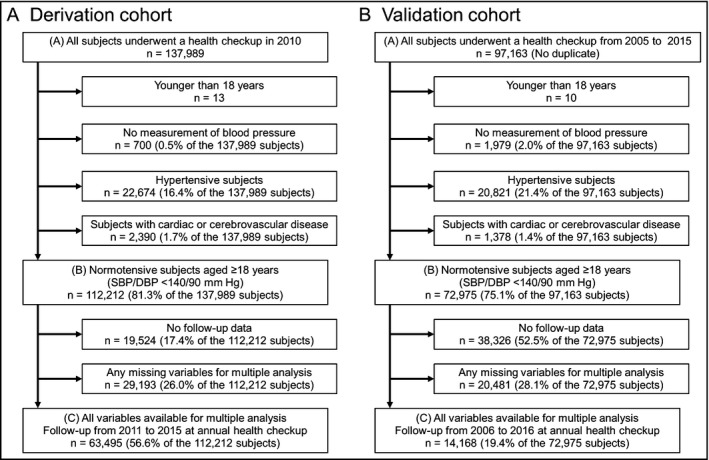
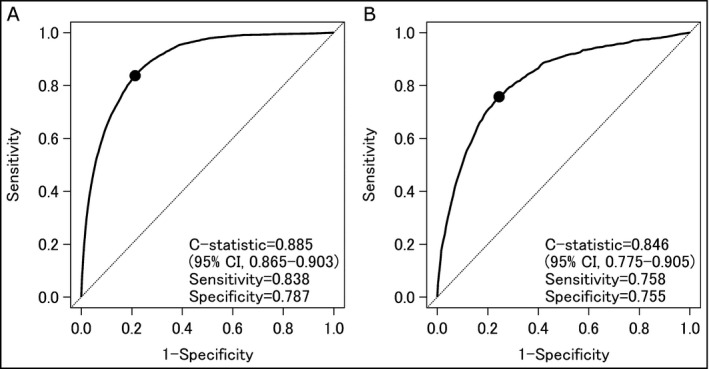
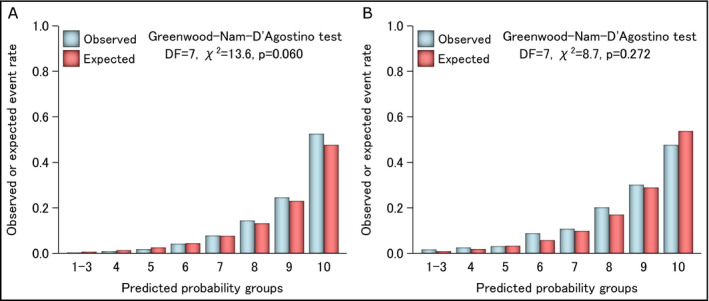
No integrated risk assessment tools that include lifestyle factors and uric acid have been developed. In accordance with the Industrial Safety and Health Law in Japan, a follow-up examination of 63 495 normotensive individuals (mean age 42.8 years) who underwent a health checkup in 2010 was conducted every year for 5 years. The primary endpoint was new-onset hypertension (systolic blood pressure [SBP]/diastolic blood pressure [DBP] ≥ 140/90 mm Hg and/or the initiation of antihypertensive medications with self-reported hypertension). During the mean 3.4 years of follow-up, 7402 participants (11.7%) developed hypertension. The prediction model included age, sex, body mass index (BMI), SBP, DBP, low-density lipoprotein cholesterol, uric acid, proteinuria, current smoking, alcohol intake, eating rate, DBP by age, and BMI by age at baseline and was created by using Cox proportional hazards models to calculate 3-year absolute risks. The derivation analysis confirmed that the model performed well both with respect to discrimination and calibration (n = 63 495; C-statistic = 0.885, 95% confidence interval [CI], 0.865-0.903; χ2 statistic = 13.6, degree of freedom [df] = 7). In the external validation analysis, moreover, the model performed well both in its discrimination and calibration characteristics (n = 14 168; C-statistic = 0.846; 95%CI, 0.775-0.905; χ2 statistic = 8.7, df = 7). Adding LDL cholesterol, uric acid, proteinuria, alcohol intake, eating rate, and BMI by age to the base model yielded a significantly higher C-statistic, net reclassification improvement (NRI), and integrated discrimination improvement, especially NRInon-event (NRI = 0.127, 95%CI = 0.100-0.152; NRInon-event = 0.108, 95%CI = 0.102-0.117). In conclusion, a highly precise model with good performance was developed for predicting incident hypertension using the new parameters of eating rate, uric acid, proteinuria, and BMI by age.
Keywords: derivation; eating rate; hypertension; prediction model; uric acid; validation.
©2018 Wiley Periodicals, Inc.
Conflict of interest statement
No conflicts of interest to disclose.
Figures
References
-
- World Health Organization . Global status report on noncommunicable diseases 2010. http://www.who.int/nmh/publications/ncd_report2010/en/. Accessed September 15, 2017.
-
- World Health Organization . Global health risks: mortality and burden of disease attributable to selected major risks. http://www.who.int/healthinfo/global_burden_disease/global_health_risks/en/. Accessed September 15, 2017.
-
- World Health Organization . A global brief on hypertension. http://www.who.int/cardiovascular_diseases/publications/global_brief_hyp.... Accessed September 15, 2017.
-
- Hansen TW, Staessen JA, Zhang H, et al. Cardiovascular outcome in relation to progression to hypertension in the Copenhagen MONICA cohort. Am J Hypertens. 2007;20:483‐491. - PubMed
-
- Vasan RS, Larson MG, Leip EP, et al. Assessment of frequency of progression to hypertension in non‐hypertensive participants in the Framingham Heart Study: a cohort study. Lancet. 2001;358:1682‐1686. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
