

Improved Diet Quality Associates With Reduction in Liver Fat, Particularly in Individuals With High Genetic Risk Scores for Nonalcoholic Fatty Liver Disease
- PMID: 29604292
- PMCID: PMC6035111
- DOI: 10.1053/j.gastro.2018.03.038
Improved Diet Quality Associates With Reduction in Liver Fat, Particularly in Individuals With High Genetic Risk Scores for Nonalcoholic Fatty Liver Disease
Abstract
Background & aims: Dietary modification has been recommended for treatment of nonalcoholic fatty liver disease (NAFLD), although it is not clear whether improving diet quality can prevent its development. We performed a prospective study to examine the association between diet quality change and change in liver fat. We also examined the association between genetic risk score and liver fat change in individuals with different levels of diet quality change.
Methods: Our study included 1521 participants who attended the seventh and eighth examinations (1998-2001 and 2005-2008) of the second-generation cohort or attended the first and second examinations (2002-2005 and 2008-2011) of the third-generation cohort in the Framingham Heart Study. The self-administered semiquantitative 126-item Harvard food frequency questionnaire was used to determine dietary intake in the year leading up to an examination. We assessed levels of liver fat using liver-phantom ratio (LPR) on computed tomography images from 2002 through 2005 and again from 2008 through 2011. LPR values are inversely related to liver fat: increased LPR indicates decreased liver fat. We examined associations of changes in 2 diet scores, the Mediterranean-style diet score (MDS) and Alternative Healthy Eating Index (AHEI), with changes in liver fat and new-onset fatty liver. We evaluated interactions between diet score change and a weighted genetic risk score for NAFLD, determined based on multiple single-nucleotide polymorphisms identified in genome-wide association studies of NAFLD. The primary outcome was change in LPR between baseline and follow-up measurement.
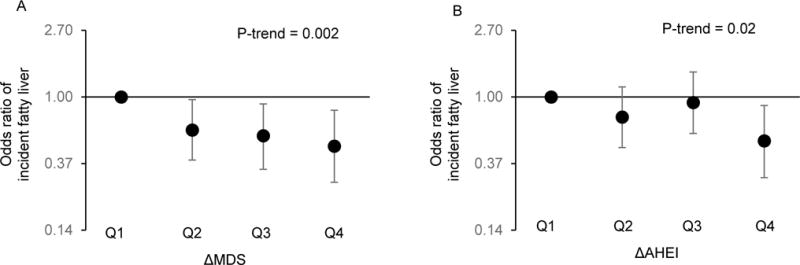
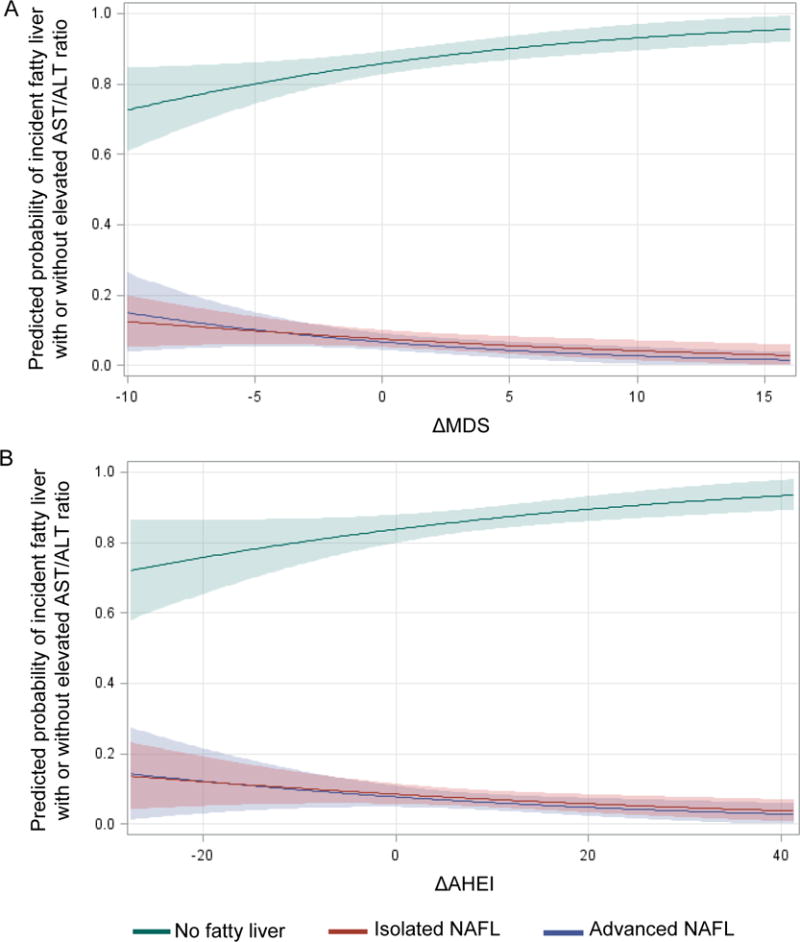
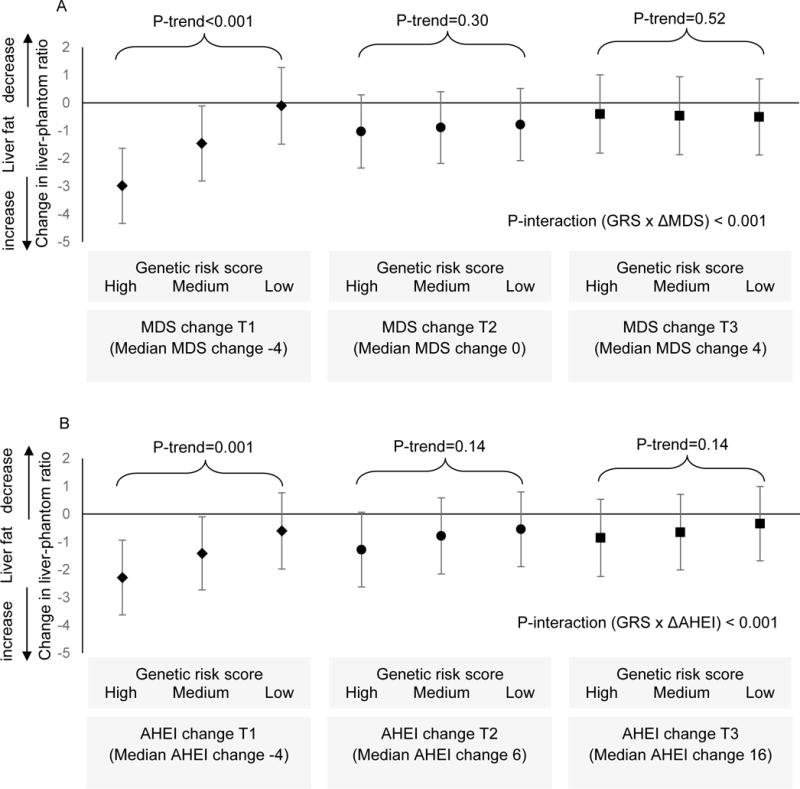
Results: For each 1 standard deviation increase in MDS, the LPR increased (meaning liver fat decreased) by 0.57 (95% confidence interval [CI] 0.27-0.86; P < .001) and the odds for incident fatty liver decreased by 26% (95% CI 10%-39%; P = .002). For each 1 standard deviation increase in AHEI, LPR increased by 0.56 (95% CI 0.29-0.84; P < .001) and the odds for incident fatty liver decreased by 21% (95% CI 5%-35%; P = .02). Increased diet scores were also associated with reduced odds of developing more-advanced fatty liver. Higher genetic risk scores were associated with increased liver fat accumulation in participants who had decreased MDS (P < .001) or AHEI scores (P = .001), but not in those with stable or improved diet scores (P for gene-diet interaction <.001).
Conclusions: In an analysis of participants in the Framingham Heart Study, increasing diet quality, determined based on MDS and AHEI scores, is associated with less liver fat accumulation and reduced risk for new-onset fatty liver. An improved diet is particularly important for individuals with a high genetic risk for NAFLD.
Keywords: Diet Quality; Fatty Liver; Prevention; Steatosis.
Copyright © 2018 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Nonalcoholic fatty liver disease (NAFLD) prevention: role of Mediterranean diet and physical activity.Hepatobiliary Surg Nutr. 2019 Apr;8(2):167-169. doi: 10.21037/hbsn.2018.12.05. Hepatobiliary Surg Nutr. 2019. PMID: 31098370 Free PMC article. No abstract available.
-
Diet quality and nonalcoholic fatty liver disease.Hepatobiliary Surg Nutr. 2019 Jun;8(3):262-263. doi: 10.21037/hbsn.2018.12.14. Hepatobiliary Surg Nutr. 2019. PMID: 31245408 Free PMC article. No abstract available.
References
-
- Rinella ME. Nonalcoholic fatty liver disease: a systematic review. JAMA. 2015;313:2263–73. - PubMed
-
- Williams CD, Stengel J, Asike MI, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology. 2011;140:124–31. - PubMed
-
- Wong RAM, Cheung R, Perumpail RB, Harrison SA, Younossi ZM, Ahmed A. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology. 2015;148:547–55. - PubMed
-
- Charlton M. Nonalcoholic fatty liver disease: a review of current understanding and future impact. Clin Gastroenterol Hepatol. 2004;2:1048–58. - PubMed
-
- Targher G, Byrne CD, Lonardo A, et al. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J Hepatol. 2016;65:589–600. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
