

The Role of the Size and Location of the Tumors and of the Vertebral Anatomy in Determining the Structural Stability of the Metastatically Involved Spine: a Finite Element Study
- PMID: 29604509
- PMCID: PMC6054594
- DOI: 10.1016/j.tranon.2018.03.002
The Role of the Size and Location of the Tumors and of the Vertebral Anatomy in Determining the Structural Stability of the Metastatically Involved Spine: a Finite Element Study
Abstract
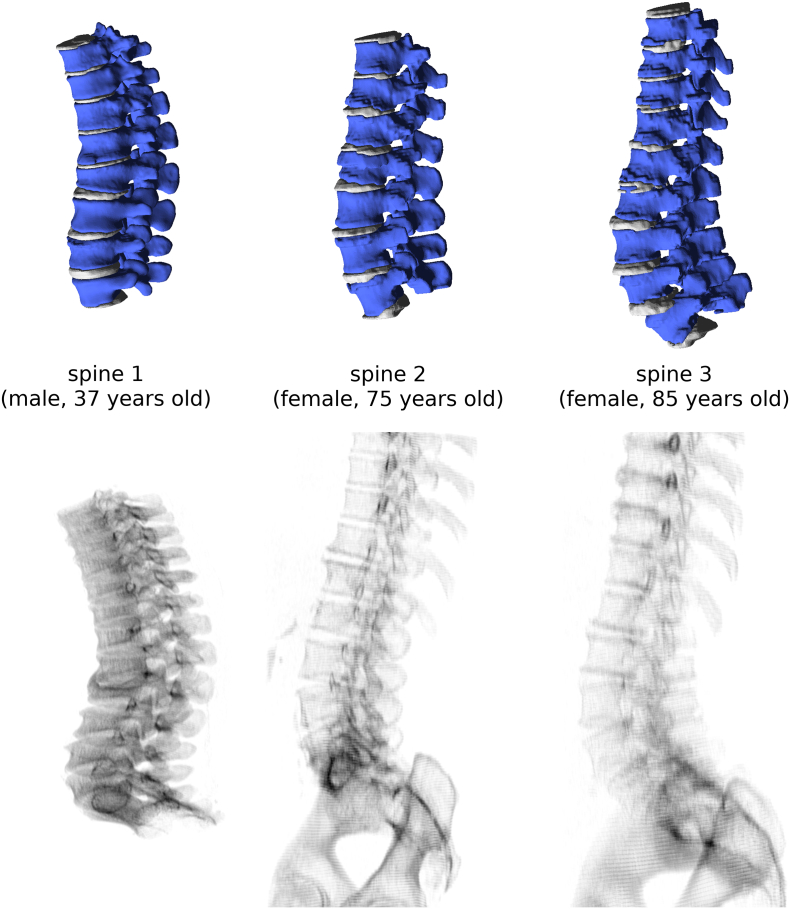
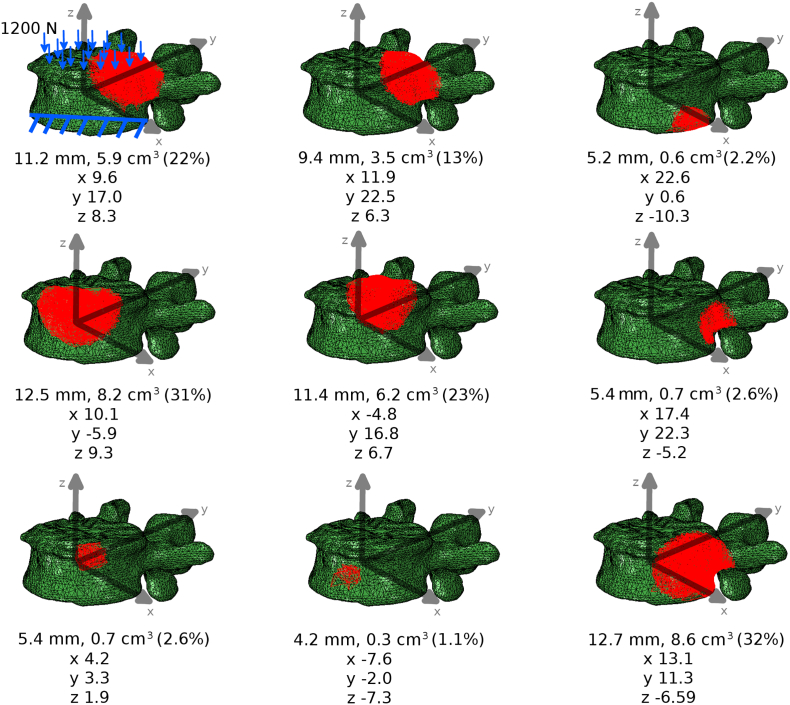
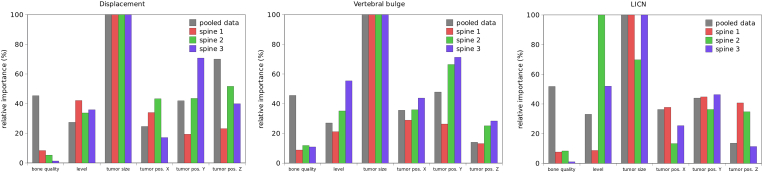
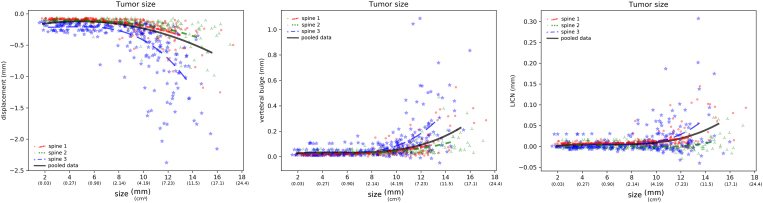
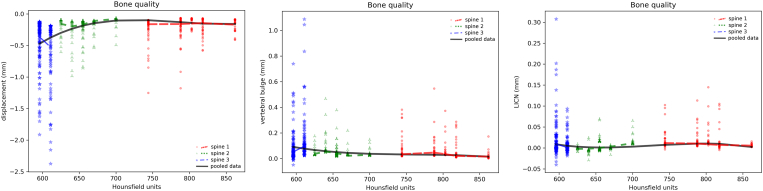
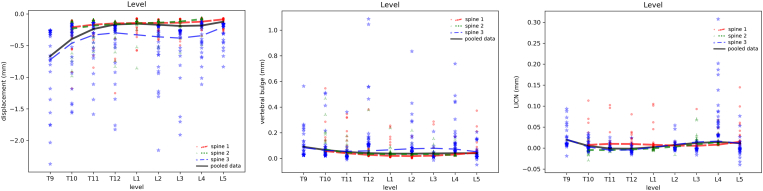
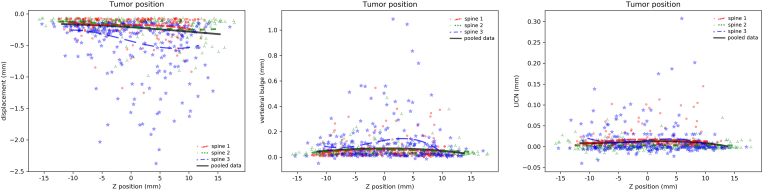
Vertebral fractures associated with the loss of structural integrity of neoplastic vertebrae are common, and determined to the deterioration of the bone quality in the lesion area. The prediction of the fracture risk in metastatically involved spines can guide in deciding if preventive solutions, such as medical prophylaxis, bracing, or surgery are indicated for the patient. In this study, finite element models of 22 thoracolumbar vertebrae were built based on CT scans of three spines, covering a wide spectrum of possible clinical scenarios in terms of age, bone quality and degenerative features, taking into account the local material properties of bone tissue. Simulations were performed in order to investigate the effect of the size and location of the tumoral lesion, the bone quality and the vertebral level in determining the structural stability of the neoplastic vertebrae. Tumors with random size and positions were added to the models, for a total of 660 simulations in which a compressive load was simulated. Results highlighted the fundamental role of the tumor size, whereas the other parameters had a lower, but non-negligible impact on the axial collapse of the vertebra, the vertebral bulge in the transverse plane and the canal narrowing under the application of the load. All the considered parameters are radiologically measurable, and can therefore be translated in a straightforward way to the clinical practice to support decisions about preventive treatment of metastatic fractures.
Copyright © 2018. Published by Elsevier Inc.
Figures
Similar articles
-
Burst fracture in the metastatically involved spine: development, validation, and parametric analysis of a three-dimensional poroelastic finite-element model.Spine (Phila Pa 1976). 2003 Apr 1;28(7):652-60. doi: 10.1097/01.BRS.0000051910.97211.BA. Spine (Phila Pa 1976). 2003. PMID: 12671351
-
Biomechanical assessment of stability in the metastatic spine following percutaneous vertebroplasty: effects of cement distribution patterns and volume.J Biomech. 2005 Aug;38(8):1582-90. doi: 10.1016/j.jbiomech.2004.07.023. J Biomech. 2005. PMID: 15958214
-
Parametric finite element analysis of vertebral bodies affected by tumors.J Biomech. 2001 Oct;34(10):1317-24. doi: 10.1016/s0021-9290(01)00086-0. J Biomech. 2001. PMID: 11522311
-
Long-term effects of vertebroplasty: adjacent vertebral fractures.J Long Term Eff Med Implants. 2006;16(4):265-80. doi: 10.1615/jlongtermeffmedimplants.v16.i4.10. J Long Term Eff Med Implants. 2006. PMID: 17073569 Review.
-
Biomechanics of metastatic disease in the vertebral column.Neurol Res. 2014 Jun;36(6):493-501. doi: 10.1179/1743132814Y.0000000362. Epub 2014 May 5. Neurol Res. 2014. PMID: 24797237 Review.
Cited by
-
A novel approach to evaluate the effects of artificial bone focal lesion on the three-dimensional strain distributions within the vertebral body.PLoS One. 2021 Jun 1;16(6):e0251873. doi: 10.1371/journal.pone.0251873. eCollection 2021. PLoS One. 2021. PMID: 34061879 Free PMC article.
-
A finite element study of the effect of cross-link stabilisation in a lumbar spine tumour model.Proc Inst Mech Eng H. 2025 Jul;239(7):607-623. doi: 10.1177/09544119251348279. Epub 2025 Jul 7. Proc Inst Mech Eng H. 2025. PMID: 40624907 Free PMC article.
-
Finite element study of sagittal fracture location on thoracolumbar fracture treatment.Front Bioeng Biotechnol. 2023 Aug 7;11:1229218. doi: 10.3389/fbioe.2023.1229218. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37609110 Free PMC article.
-
Poroelastic Characterization of Human Vertebral Metastases to Inform a Transdisciplinary Assessment of Spinal Tumors.J Clin Med. 2025 Apr 23;14(9):2913. doi: 10.3390/jcm14092913. J Clin Med. 2025. PMID: 40363945 Free PMC article.
-
Effect of size and location of simulated lytic lesions on the structural properties of human vertebral bodies, a micro-finite element study.Bone Rep. 2020 Mar 9;12:100257. doi: 10.1016/j.bonr.2020.100257. eCollection 2020 Jun. Bone Rep. 2020. PMID: 32551335 Free PMC article.
References
-
- Wilartratsami S, Muangsomboon S, Benjarassameroj S, Phimolsarnti R, Chavasiri C, Luksanapruksa P. Prevalence of primary spinal tumors: 15-year data from Siriraj Hospital. J Med Assoc Thai. 2014;97(Suppl 9):S83–7. - PubMed
-
- Boos N, Aebi M. Springer; Heidelberg: 2008. Spinal Disorders - Fundamentals of Diagnosis and Treatment.
-
- Brihaye J, Ectors P, Lemort M, Van Houtte P. The management of spinal epidural metastases. Adv Tech Stand Neurosurg. 1988;16:121–176. - PubMed
-
- Vassiliou V, Kalogeropoulou C, Petsas T, Leotsinidis M, Kardamakis D. Clinical and radiological evaluation of patients with lytic, mixed and sclerotic bone metastases from solid tumors: is there a correlation between clinical status of patients and type of bone metastases? Clin Exp Metastasis. 2007;24:49–56. - PubMed
-
- Whyne CM. Biomechanics of metastatic disease in the vertebral column. Neurol Res. 2014;36:493–501. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
