

Stereotactic ablative radiotherapy for ultra-central lung tumors: prioritize target coverage or organs at risk?
- PMID: 29606150
- PMCID: PMC5880025
- DOI: 10.1186/s13014-018-1001-6
Stereotactic ablative radiotherapy for ultra-central lung tumors: prioritize target coverage or organs at risk?
Abstract
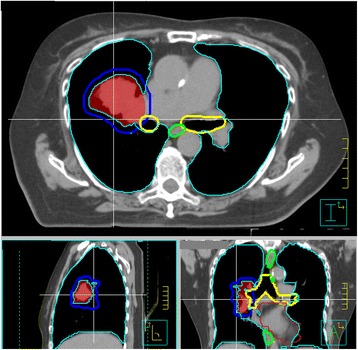
Background: Lung stereotactic ablative radiotherapy (SABR) is associated with low morbidity, however there is an increased risk of treatment-related toxicity in tumors directly abutting or invading the proximal bronchial tree, termed 'ultra-central' tumors. As there is no consensus regarding the optimal radiotherapy treatment regimen for these tumors, we performed a modeling study to evaluate the trade-offs between predicted toxicity and local control for commonly used high-precision dose-fractionation regimens.
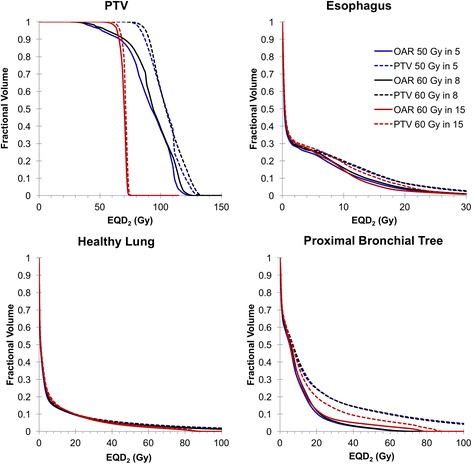
Methods: Ten patients with ultra-central lung tumors were identified from our institutional database. New plans were generated for 3 different hypofractionated schemes: 50 Gy in 5 fractions, 60 Gy in 8 fractions and 60 Gy in 15 fractions. For each regimen, one plan was created that prioritized planning target volume (PTV) coverage, potentially at the expense of organ at risk (OAR) tolerance, and a second that compromised PTV coverage to respect OAR dose constraints. Published radiobiological models were employed to evaluate competing treatment plans based on estimates for local control and the likelihood for toxicity to OAR.
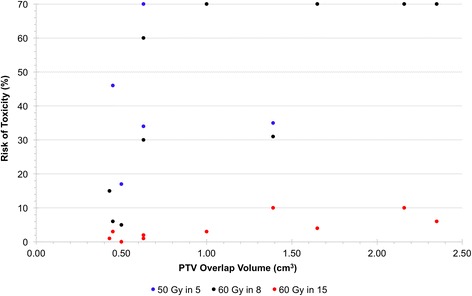
Results: The risk of esophageal or pulmonary toxicity was low (< 5%) in all scenarios. When PTV coverage was prioritized, tumor control probabilities were 92.9% for 50 Gy in 5 fractions, 92.4% for 60 Gy in 8 fractions, and 52.0% for 60 Gy in 15 fractions; however the estimated risk of grade ≥ 4 toxicity to the proximal bronchial tree was 68%, 44% and 2% respectively. When dose to OAR was prioritized, the risk of major pulmonary toxicity was reduced to < 1% in all schemes, but this compromise reduced tumor control probability to 60.3% for 50 Gy in 5 fractions, 65.7% for 60 Gy in 8 fractions and 47.8% for 60 Gy in 15 fractions.
Conclusions: The tradeoff between local control and central airway toxicity are considerable in the use of 3 commonly used hypofractionated radiotherapy regimens for ultra-central lung cancer. The results of this planning study predict that the best balance may be achieved with 60 Gy in 8 fractions compromising PTV coverage as required to maintain acceptable doses to OAR. A prospective phase I trial (SUNSET) is planned to further evaluate this challenging clinical scenario.
Keywords: Normal tissue complication probability; Stereotactic ablative radiotherapy; Ultra-central lung tumor.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the institutional research ethics board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Role of On-Table Plan Adaptation in MR-Guided Ablative Radiation Therapy for Central Lung Tumors.Int J Radiat Oncol Biol Phys. 2019 Jul 15;104(4):933-941. doi: 10.1016/j.ijrobp.2019.03.035. Epub 2019 Mar 28. Int J Radiat Oncol Biol Phys. 2019. PMID: 30928360
-
Assessment of Monte Carlo algorithm for compliance with RTOG 0915 dosimetric criteria in peripheral lung cancer patients treated with stereotactic body radiotherapy.J Appl Clin Med Phys. 2016 May 8;17(3):277-293. doi: 10.1120/jacmp.v17i3.6077. J Appl Clin Med Phys. 2016. PMID: 27167284 Free PMC article.
-
Critical structure sparing in stereotactic ablative radiotherapy for central lung lesions: helical tomotherapy vs. volumetric modulated arc therapy.PLoS One. 2013;8(4):e59729. doi: 10.1371/journal.pone.0059729. Epub 2013 Apr 5. PLoS One. 2013. PMID: 23577071 Free PMC article.
-
Increasing the Therapeutic Ratio of Stereotactic Ablative Radiotherapy by Individualized Isotoxic Dose Prescription.J Natl Cancer Inst. 2015 Oct 16;108(2):djv305. doi: 10.1093/jnci/djv305. Print 2016 Feb. J Natl Cancer Inst. 2015. PMID: 26476075 Review.
-
Safety and Effectiveness of Stereotactic Ablative Radiotherapy for Ultra-Central Lung Lesions: A Systematic Review.J Thorac Oncol. 2019 Aug;14(8):1332-1342. doi: 10.1016/j.jtho.2019.04.018. Epub 2019 May 7. J Thorac Oncol. 2019. PMID: 31075543
Cited by
-
Survival and Prognostic Factors of Ultra-Central Tumors Treated with Stereotactic Body Radiotherapy.Cancers (Basel). 2022 Nov 29;14(23):5908. doi: 10.3390/cancers14235908. Cancers (Basel). 2022. PMID: 36497390 Free PMC article.
-
And Yet It Moves: Clinical Outcomes and Motion Management in Stereotactic Body Radiation Therapy (SBRT) of Centrally Located Non-Small Cell Lung Cancer (NSCLC): Shedding Light on the Internal Organ at Risk Volume (IRV) Concept.Cancers (Basel). 2024 Jan 4;16(1):231. doi: 10.3390/cancers16010231. Cancers (Basel). 2024. PMID: 38201658 Free PMC article.
-
A single institutional experience with central lung stereotactic body radiation therapy demonstrating encouraging results with increased inter-fraction time.J Thorac Dis. 2021 Feb;13(2):642-652. doi: 10.21037/jtd-20-2659. J Thorac Dis. 2021. PMID: 33717537 Free PMC article.
-
Comparative Evaluation of 4-Dimensional Computed Tomography and 4-Dimensional Magnetic Resonance Imaging to Delineate the Target of Primary Liver Cancer.Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211045499. doi: 10.1177/15330338211045499. Technol Cancer Res Treat. 2021. PMID: 34617855 Free PMC article.
-
Dosimetric and biological comparisons of single planning and double plannings for bilateral lung cancer SBRT planning based on the Cyber-Knife system.Front Oncol. 2022 Nov 21;12:1015999. doi: 10.3389/fonc.2022.1015999. eCollection 2022. Front Oncol. 2022. PMID: 36483053 Free PMC article.
References
-
- NRG Oncology . RTOG 0236 a phase II trial of stereotactic body radiation therapy (SBRT) in the treatment of patients with medically inoperable stage I/II non-small cell lung Cancer. 2009.
-
- NRG Oncology . RTOG 0813 seamless phase I/II study of stereotactic lung radiotherapy (SBRT) for early stage, centrally located, non-small cell lung cancer (NSCLC) in medically inoperable patients. 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
