

Rituximab in the Treatment of Interstitial Lung Disease Associated with Antisynthetase Syndrome: A Multicenter Retrospective Case Review
- PMID: 29606668
- PMCID: PMC5984657
- DOI: 10.3899/jrheum.170541
Rituximab in the Treatment of Interstitial Lung Disease Associated with Antisynthetase Syndrome: A Multicenter Retrospective Case Review
Abstract
Objective: To assess clinical outcomes including imaging findings on computed tomography (CT), pulmonary function testing (PFT), and glucocorticoid (GC) use in patients with the antisynthetase syndrome (AS) and interstitial lung disease (ILD) treated with rituximab (RTX).
Methods: We retrospectively identified all patients at 2 institutions with AS-ILD who were treated with RTX. Baseline demographics, PFT, and chest CT were assessed before and after RTX. Two radiologists independently evaluated CT using a standardized scoring system.
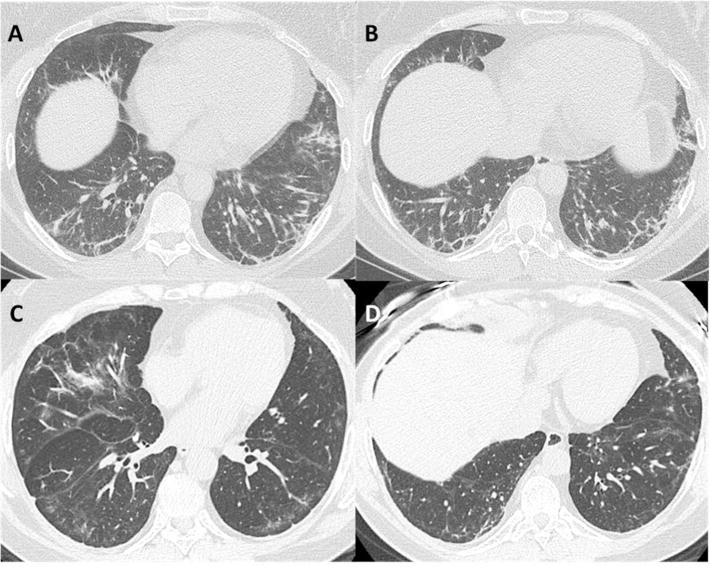
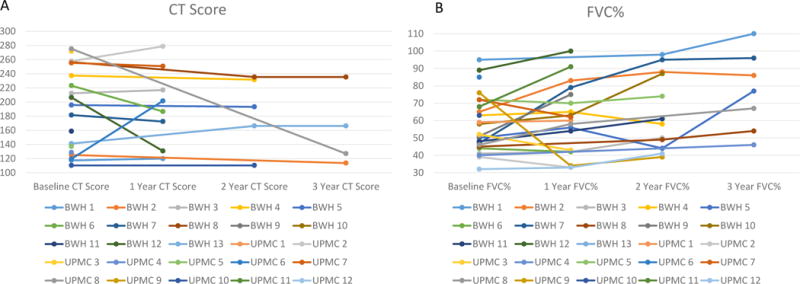
Results: Twenty-five subjects at the Brigham and Women's Hospital (n = 13) and University of Pittsburgh Medical Center (n = 12) were included. Antisynthetase antibodies were identified in all patients (16 Jo1, 6 PL-12, 3 PL-7). In 21 cases (84%), the principal indication for RTX use was recurrent or progressive ILD, owing to failure of other agents. Comparing pre- and post-RTX pulmonary variables at 12 months, CT score and forced vital capacity were stable or improved in 88% and 79% of subjects, respectively. Total lung capacity (%) increased from 56 ± 13 to 64 ± 13 and GC dose decreased from 18 ± 9 to 12 ± 12 mg/day. Although DLCO (%) declined slightly at 1 year, it increased from 42 ± 17 to 70 ± 20 at 3 years. The most common imaging patterns on CT were nonspecific interstitial pneumonia (NSIP; n = 13) and usual interstitial pneumonia/fibrotic NSIP (n = 5), of which 5 had concurrent elements of cryptogenic organizing pneumonia.
Conclusion: Stability or improvement in pulmonary function or severity of ILD on CT was seen in most patients. Use of RTX was well tolerated in the majority of patients. RTX may play a therapeutic role in patients with AS-ILD, and further clinical investigation is warranted.
Keywords: ANTISYNTHETASE SYNDROME; INTERSTITIAL LUNG DISEASE; RITUXIMAB.
Figures
References
-
- Katzap E, Barilla-LaBarca ML, Marder G. Antisynthetase syndrome. Curr Rheumatol Rep. 2011;13:175–181. - PubMed
-
- Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts) N Engl J Med. 1975;292:344–347. - PubMed
-
- Connors GR, Christopher-Stine L, Oddis CV, Danoff SK. Interstitial lung disease associated with the idiopathic inflammatory myopathies: What progress has been made in the past 35 years? Chest. 2010;138:1464–1474. - PubMed
-
- Hallowell RW, Danoff SK. Interstitial lung disease associated with the idiopathic inflammatory myopathies and the antisynthetase syndrome: Recent advances. Curr Opin Rheumatol. 2014;26:684–689. - PubMed
-
- Marie I, Hatron PY, Dominique S, Cherin P, Mouthon L, Menard JF. Short-term and long-term outcomes of interstitial lung disease in polymyositis and dermatomyositis: A series of 107 patients. Arthritis Rheum. 2011;63:3439–3447. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous