

Overview of Current Concepts in Gastric Intestinal Metaplasia and Gastric Cancer
- PMID: 29606921
- PMCID: PMC5866308
Overview of Current Concepts in Gastric Intestinal Metaplasia and Gastric Cancer
Abstract
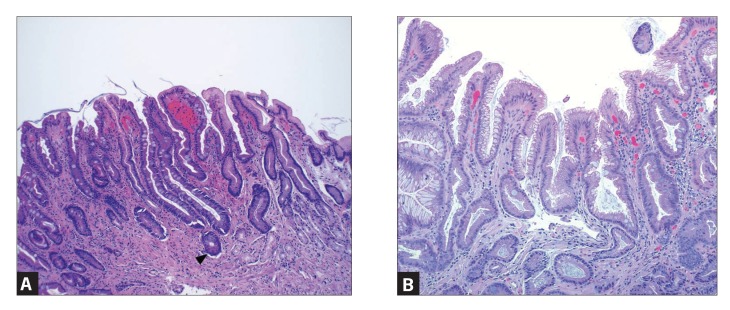
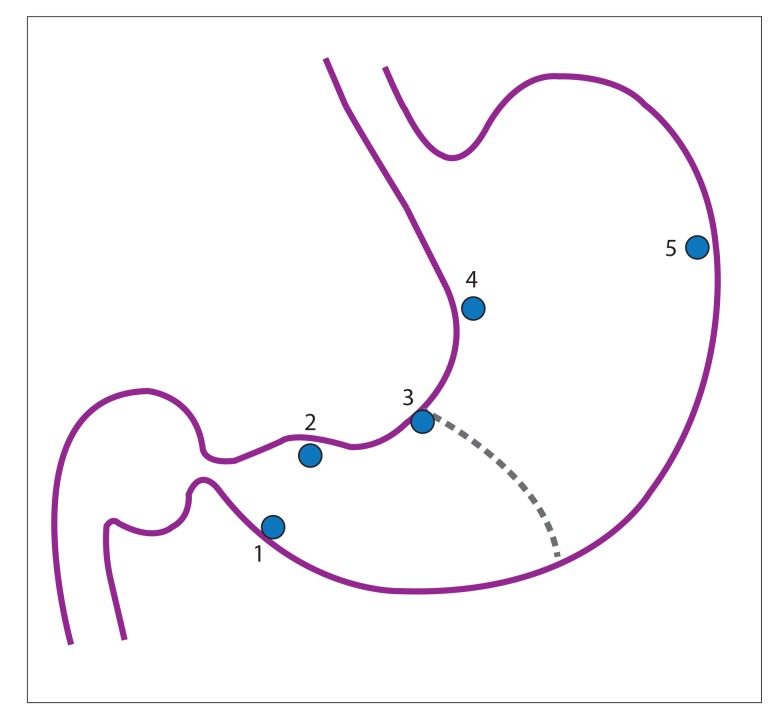
Gastric intestinal metaplasia is a precancerous change of the mucosa of the stomach with intestinal epithelium, and is associated with an increased risk of dysplasia and cancer. The pathogenesis to gastric cancer is proposed by the Correa hypothesis as the transition from normal gastric epithelium to invasive cancer via inflammation followed by intramucosal cancer and invasion. Multiple risk factors have been associated with the development of gastric intestinal metaplasia interplay, including Helicobacter pylori infection and associated genomics, host genetic factors, environmental milieu, rheumatologic disorders, diet, and intestinal microbiota. Globally, screening guidelines have been established in countries with high incidence. In the United States, no such guidelines have been developed due to lower, albeit increasing, incidence. The American Society for Gastrointestinal Endoscopy recommends a case-by-case patient assessment based upon epidemiology, genetics, and environmental risk factors. Studies have examined the use of a serologic biopsy to stratify risk based upon factors such as H pylori status and virulence factors, along with serologic markers of chronic inflammation including pepsinogen I, pepsinogen II, and gastrin. High-risk patients may then be advised to undergo endoscopic evaluation with mapping biopsies from the antrum (greater curvature, lesser curvature), incisura angularis, and corpus (greater curvature, lesser curvature). Surveillance guidelines have not been firmly established for patients with known gastric intestinal metaplasia, but include repeat endoscopy at intervals according to the histologic risk for malignant transformation.
Keywords: Gastric intestinal metaplasia; Helicobacter pylori; gastric cancer surveillance; intestinal-type gastric cancer; serologic biopsy; spasmolytic polypeptide-expressing metaplasia.
Conflict of interest statement
The authors wish to thank Brian Theisen, MD, for providing the pathology figures and caption. The authors have no relevant conflicts of interest to disclose.
Figures
Similar articles
-
AGA Clinical Practice Update on the Diagnosis and Management of Atrophic Gastritis: Expert Review.Gastroenterology. 2021 Oct;161(4):1325-1332.e7. doi: 10.1053/j.gastro.2021.06.078. Epub 2021 Aug 26. Gastroenterology. 2021. PMID: 34454714 Free PMC article. Review.
-
Intestinal metaplasia of the gastric cardia: a study from Turkey.Hepatogastroenterology. 2002 Jul-Aug;49(46):1153-6. Hepatogastroenterology. 2002. PMID: 12143225
-
Histologic and serum risk markers for noncardia early gastric cancer.Int J Cancer. 2005 Jun 20;115(3):463-9. doi: 10.1002/ijc.20852. Int J Cancer. 2005. PMID: 15688378
-
Antral-type mucosa in the gastric incisura, body, and fundus (antralization): a link between Helicobacter pylori infection and intestinal metaplasia?Am J Gastroenterol. 2000 Jan;95(1):114-21. doi: 10.1111/j.1572-0241.2000.01609.x. Am J Gastroenterol. 2000. PMID: 10638568
-
Gastric atrophy, metaplasia, and dysplasia: a clinical perspective.J Clin Gastroenterol. 2003 May-Jun;36(5 Suppl):S29-36; discussion S61-2. doi: 10.1097/00004836-200305001-00006. J Clin Gastroenterol. 2003. PMID: 12702963 Review.
Cited by
-
Modified Chaishao Liujunzi Decoction inhibits bile acid-induced gastric intestinal metaplasia: from network prediction to experimental verification.Aging (Albany NY). 2023 Dec 10;15(23):13998-14018. doi: 10.18632/aging.205285. Epub 2023 Dec 10. Aging (Albany NY). 2023. PMID: 38096029 Free PMC article.
-
The immune microenvironment in gastric adenocarcinoma.Nat Rev Gastroenterol Hepatol. 2022 Jul;19(7):451-467. doi: 10.1038/s41575-022-00591-0. Epub 2022 Mar 14. Nat Rev Gastroenterol Hepatol. 2022. PMID: 35288702 Free PMC article. Review.
-
Gastrointestinal Cancer Precursor Conditions and Their Detection.Hematol Oncol Clin North Am. 2024 Aug;38(4):783-811. doi: 10.1016/j.hoc.2024.04.002. Epub 2024 May 17. Hematol Oncol Clin North Am. 2024. PMID: 38760197 Free PMC article. Review.
-
Novel In Vivo Mouse Cryoablation Model to Explore Unique Therapeutic Approaches for Premalignant Columnar Lesions.Methods Protoc. 2021 Jan 5;4(1):6. doi: 10.3390/mps4010006. Methods Protoc. 2021. PMID: 33526760 Free PMC article.
-
Multi-bioinformatics revealed potential biomarkers and repurposed drugs for gastric adenocarcinoma-related gastric intestinal metaplasia.NPJ Syst Biol Appl. 2024 Nov 4;10(1):127. doi: 10.1038/s41540-024-00455-0. NPJ Syst Biol Appl. 2024. PMID: 39496635 Free PMC article.
References
-
- Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ American Gastroenterological Association. American Gastroenterological Association medical position statement on the management of Barrett’s esophagus. Gastroenterology. 2011;140(3):1084–1091. - PubMed
-
- Howlader N, Noone AM, Krapcho M, et al. SEER cancer statistics review, 1975-2014 National Cancer Institute. [Accessed January 23, 2018]. https://seer.cancer.gov/csr/1975_2014/ eds. Published April 2017. Updated June 28, 2017.
-
- International Agency for Research on Cancer, World Health Organization. GLOBOCAN 2012: estimated cancer incidence, mortality and prevalence worldwide in 2012. [Accessed January 23, 2018]. http://globocan.iarc.fr/Default.aspx
LinkOut - more resources
Full Text Sources
Medical