

Prognosis of multi-level N2-positive non-small cell lung cancer according to lymph node staging using endobronchial ultrasound-transbronchial biopsy
- PMID: 29607613
- PMCID: PMC5983197
- DOI: 10.1111/1759-7714.12629
Prognosis of multi-level N2-positive non-small cell lung cancer according to lymph node staging using endobronchial ultrasound-transbronchial biopsy
Abstract
Background: The optimal treatment for stage IIIA-N2 non-small cell lung cancer (NSCLC) remains controversial, and multidisciplinary team approaches are needed. Downstaging after induction therapy is a good prognostic factor in surgical patients; however, re-evaluation of nodal status before surgery is challenging. The aim of this study was to evaluate the prognosis of patients with multi-level N2 NSCLC who received surgery or chemoradiation therapy (CRT) according to restaging using endobronchial ultrasound-transbronchial aspiration (EBUS-TBNA).
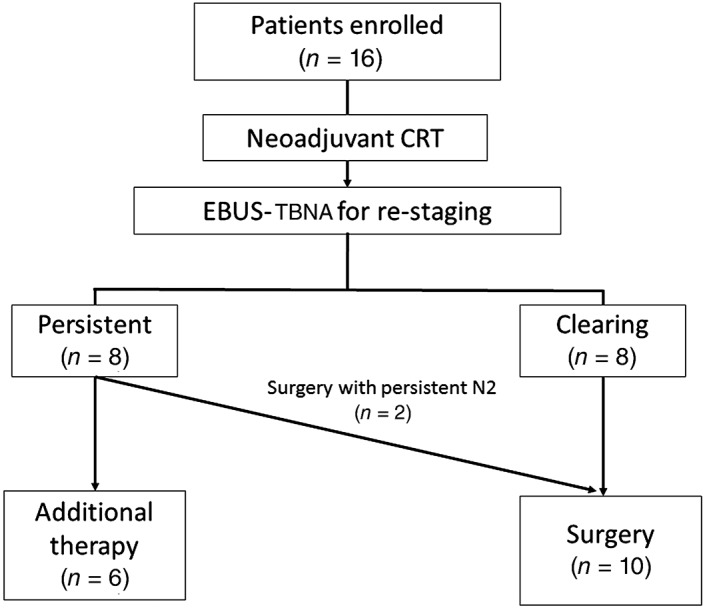
Methods: This was a single center, prospective study that included 16 patients with biopsy-proven multi-level N2 disease on initial EBUS-TBNA that was restaged using EBUS-TBNA after induction therapy. Cases downstaged after rebiopsy were treated surgically. Three-year progression-free survival (PFS) and locoregional PFS were determined using Kaplan-Meier analysis.
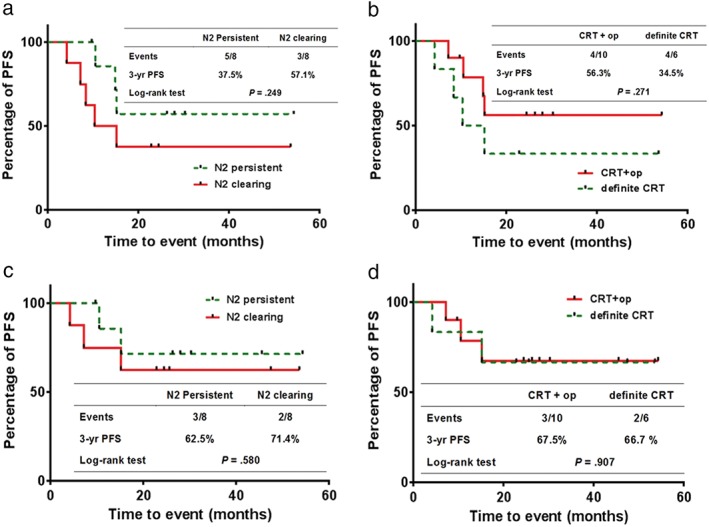
Results: Of the 16 patients (median age 58 years, male 63%), eight had persistent N2 disease and eight showed N2 clearance on restaging using EBUS-TBNA. Ten patients underwent surgery, including two patients without N2 clearance. Recurrence and locoregional recurrence occurred in eight and five patients, respectively. The three-year PFS was longer in patients with N2 clearance than in those with N2 persistent disease (57.1% vs. 37.5%). Patients with N2 clearance also had longer three-year locoregional PFS than those with N2 persistent disease (71.4% vs. 62.5%).
Conclusions: EBUS-TBNA could be an effective diagnostic method for restaging in multi-level N2 NSCLC patients after induction CRT. As this was a pilot study, further large-scale randomized studies are needed.
Keywords: Downstaging; endobronchial ultrasound-transbronchial aspiration; multimodality treatment; neoadjuvant therapy; non-small cell lung cancer.
© 2018 The Authors. Thoracic Cancer published by China Lung Oncology Group and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Endobronchial ultrasound-guided transbronchial needle aspiration validated with video-assisted mediastinoscopic lymphadenectomy in the mediastinal restaging of patients with stage IIIA non-small cell lung cancer after induction therapy.Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666241301284. doi: 10.1177/17534666241301284. Ther Adv Respir Dis. 2024. PMID: 39604280 Free PMC article.
-
Endobronchial ultrasound with transbronchial needle aspiration for restaging the mediastinum in lung cancer.J Clin Oncol. 2008 Jul 10;26(20):3346-50. doi: 10.1200/JCO.2007.14.9229. Epub 2008 Jun 2. J Clin Oncol. 2008. PMID: 18519953
-
Endobronchial ultrasound-transbronchial needle aspiration: effectiveness and accuracy in non-small cell lung cancer staging.Updates Surg. 2024 Sep;76(5):1909-1918. doi: 10.1007/s13304-024-01777-8. Epub 2024 Mar 11. Updates Surg. 2024. PMID: 38466540
-
Endosonography with lymph node sampling for restaging the mediastinum in lung cancer: A systematic review and pooled data analysis.J Thorac Cardiovasc Surg. 2020 Mar;159(3):1099-1108.e5. doi: 10.1016/j.jtcvs.2019.07.095. Epub 2019 Aug 28. J Thorac Cardiovasc Surg. 2020. PMID: 31590952
-
Preoperative Staging by EBUS in cN0/N1 Lung Cancer: Systematic Review and Meta-Analysis.J Bronchology Interv Pulmonol. 2019 Jul;26(3):155-165. doi: 10.1097/LBR.0000000000000545. J Bronchology Interv Pulmonol. 2019. PMID: 30119069
Cited by
-
Report of the Korean Association of Lung Cancer Registry (KALC-R), 2014.Cancer Res Treat. 2019 Oct;51(4):1400-1410. doi: 10.4143/crt.2018.704. Epub 2019 Feb 25. Cancer Res Treat. 2019. PMID: 30913875 Free PMC article.
-
18F-fluorodeoxyglucose positron emission tomography/computed tomography in the evaluation of clinically node-negative non-small cell lung cancer.Thorac Cancer. 2019 Mar;10(3):413-420. doi: 10.1111/1759-7714.12978. Epub 2019 Jan 21. Thorac Cancer. 2019. PMID: 30666803 Free PMC article. Review.
References
-
- Albain KS, Rusch VW, Crowley JJ et al Concurrent cisplatin/etoposide plus chest radiotherapy followed by surgery for stages IIIA (N2) and IIIB non‐small‐cell lung cancer: Mature results of Southwest Oncology Group phase II study 8805. J Clin Oncol 1995; 13: 1880–92. - PubMed
-
- Elias AD, Skarin AT, Leong T et al Neoadjuvant therapy for surgically staged IIIA N2 non‐small cell lung cancer (NSCLC). Lung Cancer 1997; 17: 147–61. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
