

Pilot Study of a Device to Induce the Hanger Reflex in Patients with Cervical Dystonia
- PMID: 29607887
- PMCID: PMC5958042
- DOI: 10.2176/nmc.oa.2017-0111
Pilot Study of a Device to Induce the Hanger Reflex in Patients with Cervical Dystonia
Abstract
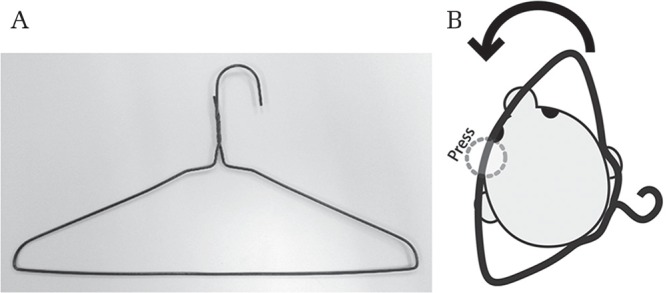
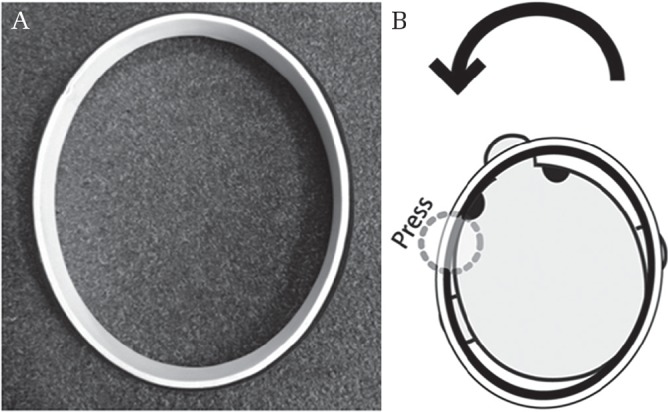
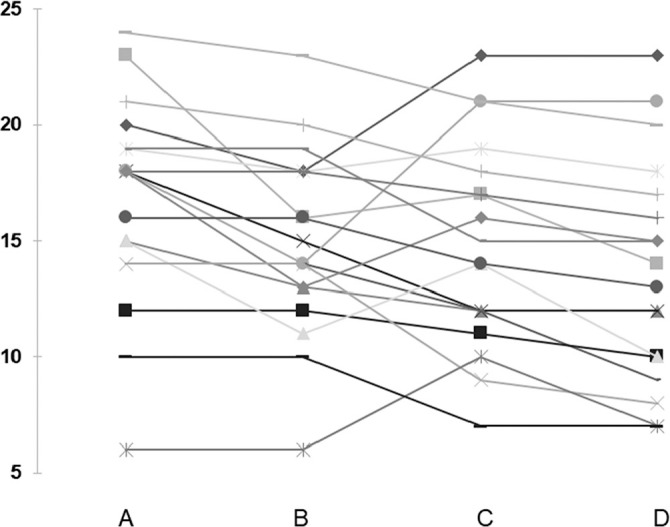
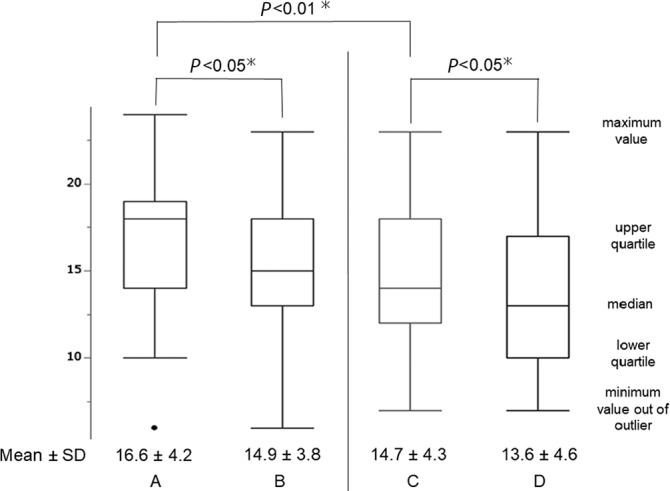
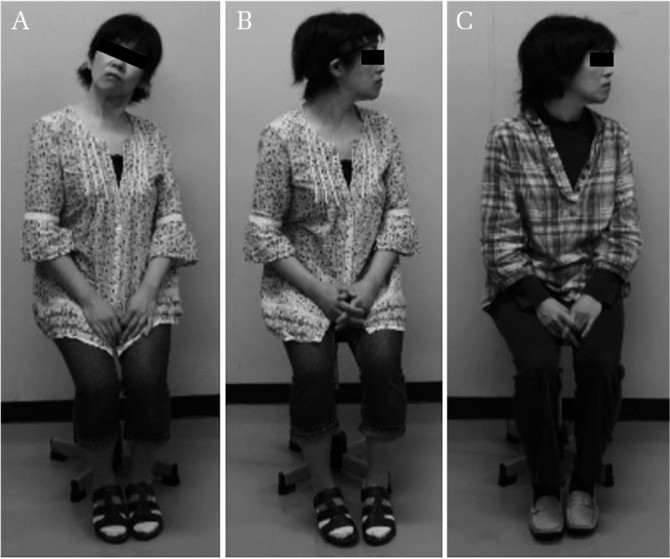
The hanger reflex (HR) is an involuntary head rotation that occurs in response to a clothes hanger encircling the head and compressing the unilateral fronto-temporal area. Here, we developed an elliptical device to induce the HR and examined its utility for the treatment of cervical dystonia (CD). The study included 19 patients with rotational-type CD. The device was applied to each subject's head for at least 30 min/day for 3 months. Severity scores on part 1 of the Toronto Western Spasmodic Torticollis Rating Scale were evaluated at baseline and after the 3-month trial. Mean scores without and with the device were significantly different both at baseline (16.6 vs. 14.7, respectively; P < 0.05) and after the trial (14.9 vs. 13.6, respectively; P < 0.05). This preliminary trial suggests that our device can improve abnormal head rotation in patients with CD.
Keywords: cervical dystonia; hanger reflex; neurorehabilitation.
Conflict of interest statement
This study was supported by JSPS KAKENHI (23791587) and a Hokugin grant for young scientists. The JSPS KAKENHI and Hokugin grant for young scientists provided unrestricted support and had no role in the oversight or review of the research data or reporting. The authors (TA, KT, MF, and SK) have registered online self-reported COI Disclosure Statement Forms through the website for the Japan Neurosurgical Society members.
Figures
Similar articles
-
The Hanger Reflex: An Inexpensive and Non-invasive Therapeutic Modality for Dystonia and Neurological Disorders.Neurol Med Chir (Tokyo). 2020 Nov 15;60(11):525-530. doi: 10.2176/nmc.ra.2020-0156. Epub 2020 Oct 16. Neurol Med Chir (Tokyo). 2020. PMID: 33071275 Free PMC article. Review.
-
Sustainable Improvement of Anterocollis-type Cervical Dystonia with a Hanger Reflex Device: A Case Report.NMC Case Rep J. 2024 Sep 21;11:263-266. doi: 10.2176/jns-nmc.2024-0146. eCollection 2024. NMC Case Rep J. 2024. PMID: 39544225 Free PMC article.
-
Rate of Hanger Reflex Occurrence: Unexpected Head Rotation on Fronto-temporal Head Compression.Neurol Med Chir (Tokyo). 2015;55(7):587-91. doi: 10.2176/nmc.oa.2014-0324. Epub 2015 Jun 29. Neurol Med Chir (Tokyo). 2015. PMID: 26119894 Free PMC article.
-
Concurrent onabotulinumtoxinA treatment of cervical dystonia and concomitant migraine.Headache. 2012 Sep;52(8):1219-25. doi: 10.1111/j.1526-4610.2012.02164.x. Epub 2012 May 18. Headache. 2012. PMID: 22607530 Clinical Trial.
-
[Cervical dystonia--diagnosis and treatment].Tidsskr Nor Laegeforen. 2008 Oct 9;128(19):2202-5. Tidsskr Nor Laegeforen. 2008. PMID: 18846145 Review. Norwegian.
Cited by
-
The Hanger Reflex: An Inexpensive and Non-invasive Therapeutic Modality for Dystonia and Neurological Disorders.Neurol Med Chir (Tokyo). 2020 Nov 15;60(11):525-530. doi: 10.2176/nmc.ra.2020-0156. Epub 2020 Oct 16. Neurol Med Chir (Tokyo). 2020. PMID: 33071275 Free PMC article. Review.
-
Sustainable Improvement of Anterocollis-type Cervical Dystonia with a Hanger Reflex Device: A Case Report.NMC Case Rep J. 2024 Sep 21;11:263-266. doi: 10.2176/jns-nmc.2024-0146. eCollection 2024. NMC Case Rep J. 2024. PMID: 39544225 Free PMC article.
-
Effects of hanger reflex on the cervical muscular activation and function: A surface electromyography assessment.Front Physiol. 2022 Oct 11;13:1006179. doi: 10.3389/fphys.2022.1006179. eCollection 2022. Front Physiol. 2022. PMID: 36311253 Free PMC article.
References
-
- Steeves TD, Day L, Dykeman J, Jette N, Pringsheim T: The prevalence of primary dystonia: a systematic review and meta-analysis. Mov Disord 27: 1789–1796, 2012 - PubMed
-
- Leis AA, Dimitrijevic MR, Delapasse JS, Sharkey PC: Modification of cervical dystonia by selective sensory stimulation. J Neurol Sci 110: 79–89, 1992 - PubMed
-
- Jahanshahi M, Sartory G, Marsden CD: EMG biofeedback treatment of torticollis: a controlled outcome study. Biofeedback Self Regul 16: 413–448, 1991 - PubMed
-
- Zetterberg L, Halvorsen K, Färnstrand C, Aquilonius SM, Lindmark B: Physiotherapy in cervical dystonia: six experimental single-case studies. Physiother Theory Pract 24: 275–290, 2008 - PubMed
-
- Smania N, Corato E, Tinazzi M, Montagnana B, Fiaschi A, Aglioti SM: The effect of two different rehabilitation treatments in cervical dystonia: preliminary results in four patients. Funct Neurol 18: 219–225, 2003 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources