

Changes In Hospital Utilization Three Years Into Maryland's Global Budget Program For Rural Hospitals
- PMID: 29608370
- PMCID: PMC5993431
- DOI: 10.1377/hlthaff.2018.0112
Changes In Hospital Utilization Three Years Into Maryland's Global Budget Program For Rural Hospitals
Abstract
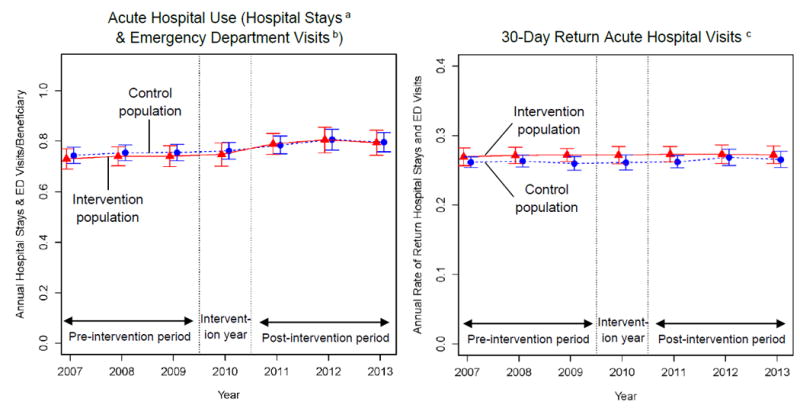
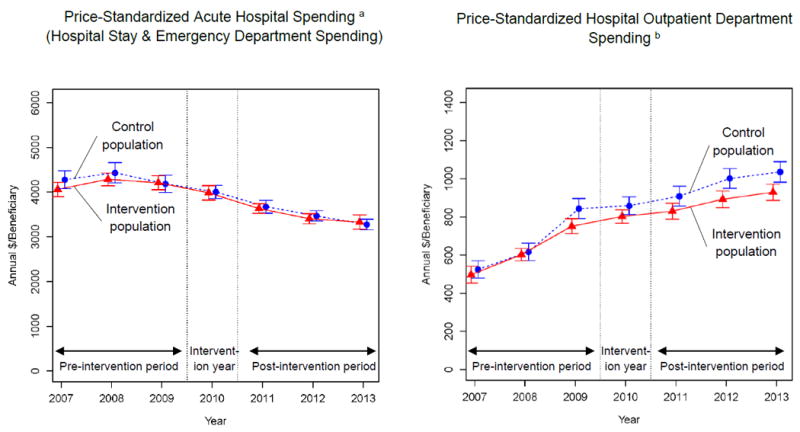
In a substantial shift in payment policy, the State of Maryland implemented a global budget program for acute care hospitals in 2010. Goals of the program include controlling hospital use and spending. Eight rural hospitals entered the program in 2010, while urban and suburban hospitals joined in 2014. Prior analyses, which focused on urban and suburban hospitals, did not find consistent evidence that Maryland's program had contributed to changes in hospital use after two years. However, these studies were limited by short follow-up periods, may have failed to isolate impacts of Maryland's payment change from other state trends, and had limited generalizability to rural settings. To understand the effects of Maryland's global budget program on rural hospitals, we compared changes in hospital use among Medicare beneficiaries served by affected rural hospitals versus an in-state control population from before to after 2010. By 2013-three years after the rural program began-there were no differential changes in acute hospital use or price-standardized hospital spending among beneficiaries served by the affected hospitals, versus the within-state control group. Our results suggest that among Medicare beneficiaries, global budgets in rural Maryland hospitals did not reduce hospital use or price-standardized spending as policy makers had anticipated.
Keywords: Health Economics; Health Reform; Hospitals; payment.
Figures
Similar articles
-
Changes in Health Care Use Associated With the Introduction of Hospital Global Budgets in Maryland.JAMA Intern Med. 2018 Feb 1;178(2):260-268. doi: 10.1001/jamainternmed.2017.7455. JAMA Intern Med. 2018. PMID: 29340564 Free PMC article.
-
Maryland's Global Hospital Budgets: Impacts on Medicare Cost and Utilization for the First 3 Years.Med Care. 2019 Jun;57(6):417-424. doi: 10.1097/MLR.0000000000001118. Med Care. 2019. PMID: 30994523
-
Maryland's Global Hospital Budgets--Preliminary Results from an All-Payer Model.N Engl J Med. 2015 Nov 12;373(20):1899-901. doi: 10.1056/NEJMp1508037. N Engl J Med. 2015. PMID: 26559570
-
Impacts of Maryland's Global Budgets on Medicare and Commercial Spending and Utilization.Med Care Res Rev. 2021 Dec;78(6):725-735. doi: 10.1177/1077558720954693. Epub 2020 Sep 13. Med Care Res Rev. 2021. PMID: 32924778
-
Bypassing of local hospitals by rural Medicare beneficiaries.J Rural Health. 1994 Fall;10(4):237-46. doi: 10.1111/j.1748-0361.1994.tb00237.x. J Rural Health. 1994. PMID: 10139173 Review.
Cited by
-
Global budget versus cost ceiling: a natural experiment in hospital payment reform in the Netherlands.Eur J Health Econ. 2020 Feb;21(1):105-114. doi: 10.1007/s10198-019-01114-6. Epub 2019 Sep 16. Eur J Health Econ. 2020. PMID: 31529343 Free PMC article.
-
Influence of the Maryland All-Payer Model on Primary Total Knee Arthroplasties.JB JS Open Access. 2019 Dec 10;4(4):e0041. doi: 10.2106/JBJS.OA.19.00041. eCollection 2019 Oct-Dec. JB JS Open Access. 2019. PMID: 32043062 Free PMC article.
-
China Promotes Sanming's Model: A National Template for Integrated Medicare Payment Methods.Int J Integr Care. 2023 May 11;23(2):15. doi: 10.5334/ijic.7011. eCollection 2023 Apr-Jun. Int J Integr Care. 2023. PMID: 37188056 Free PMC article.
-
Do budget constraints limit access to health care? Evidence from PCI treatments in Hungary.Int J Health Econ Manag. 2023 Jun;23(2):281-302. doi: 10.1007/s10754-023-09349-w. Epub 2023 Apr 19. Int J Health Econ Manag. 2023. PMID: 37074540 Free PMC article.
-
Early impacts of the Pennsylvania Rural Health Model on potentially avoidable utilization.Health Aff Sch. 2024 Jan 19;2(2):qxae002. doi: 10.1093/haschl/qxae002. eCollection 2024 Feb. Health Aff Sch. 2024. PMID: 38313868 Free PMC article.
References
-
- Anderson GF, Davis K, Guterman S. Medicare Payment Reform: Aligning Incentives for Better Care. New York, NY: Commonwealth Fund; 2015. - PubMed
-
- Burwell SM. Setting Value-Based Payment Goals – HHS Efforts to Improve U.S. Health Care. New England Journal of Medicine. 2015;372(10):897–899. - PubMed
-
- Rajkumar R, Conway PH, Tavenner M. CMS-engaging multiple payers in payment reform. Jama. 2014;311(19):1967–1968. - PubMed
-
- Nyweide DJ, Lee W, Cuerdon TT, et al. Association of pioneer accountable care organizations vs traditional medicare fee for service with spending, utilization, and patient experience. Jama. 2015;313(21):2152–2161. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical