

Biomechanics of Immediate Postextraction Implant Osseointegration
- PMID: 29608868
- PMCID: PMC6055256
- DOI: 10.1177/0022034518765757
Biomechanics of Immediate Postextraction Implant Osseointegration
Abstract
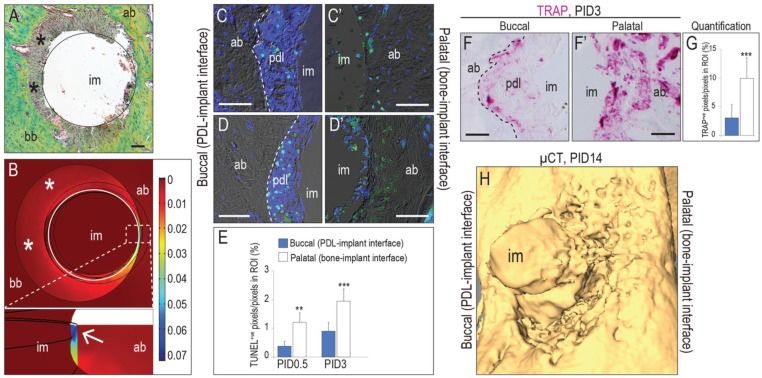
The aim of this study was to gain insights into the biology and mechanics of immediate postextraction implant osseointegration. To mimic clinical practice, murine first molar extraction was followed by osteotomy site preparation, specifically in the palatal root socket. The osteotomy was positioned such that it removed periodontal ligament (PDL) only on the palatal aspect of the socket, leaving the buccal aspect undisturbed. This strategy created 2 distinct peri-implant environments: on the palatal aspect, the implant was in direct contact with bone, while on the buccal aspect, a PDL-filled gap existed between the implant and bone. Finite element modeling showed high strains on the palatal aspect, where bone was compressed by the implant. Osteocyte death and bone resorption predominated on the palatal aspect, leading to the loss of peri-implant bone. On the buccal aspect, where finite element modeling revealed low strains, there was minimal osteocyte death and robust peri-implant bone formation. Initially, the buccal aspect was filled with PDL remnants, which we found directly provided Wnt-responsive cells that were responsible for new bone formation and osseointegration. On the palatal aspect, which was devoid of PDL and Wnt-responsive cells, adding exogenous liposomal WNT3A created an osteogenic environment for rapid peri-implant bone formation. Thus, we conclude that low strain and high Wnt signaling favor osseointegration of immediate postextraction implants. The PDL harbors Wnt-responsive cells that are inherently osteogenic, and if the PDL tissue is healthy, it is reasonable to preserve this tissue during immediate implant placement.
Keywords: Wnt3 protein; cell lineage; dental implantation; osteogenic; periodontal ligament; tooth extraction.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures



References
-
- Almeida M, Han L, Bellido T, Manolagas SC, Kousteni S. 2005. Wnt proteins prevent apoptosis of both uncommitted osteoblast progenitors and differentiated osteoblasts by beta-catenin-dependent and -independent signaling cascades involving Src/ERK and phosphatidylinositol 3-kinase/AKT. J Biol Chem. 280(50):41342–41351. - PubMed
-
- Anitua E, Pinas L, Alkhraisat MH. 2016. Long-term outcomes of immediate implant placement into infected sockets in association with immediate loading: a retrospective cohort study. J Periodontol. 87(10):1135–1140. - PubMed
-
- Branemark PI, Hansson BO, Adell R, Breine U, Lindstrom J, Hallen O, Ohman A. 1977. Osseointegrated implants in the treatment of the edentulous jaw: experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 16:1–132. - PubMed
-
- Brunski JB. 1999. In vivo bone response to biomechanical loading at the bone/dental-implant interface. Adv Dent Res. 13:99–119. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
