

Subclinical atherosclerosis, cardiovascular health, and disease risk: is there a case for the Cardiovascular Health Index in the primary prevention population?
- PMID: 29609588
- PMCID: PMC5880087
- DOI: 10.1186/s12889-018-5263-6
Subclinical atherosclerosis, cardiovascular health, and disease risk: is there a case for the Cardiovascular Health Index in the primary prevention population?
Abstract
Background: Current primary prevention guidelines for cardiovascular disease (CVD) prioritize risk identification, risk stratification using clinical and risk scores, and risk reduction with lifestyle interventions and pharmacotherapy. Subclinical atherosclerosis is an early indicator of atherosclerotic burden and its timely recognition can slow or prevent progression to CVD. Thus, individuals with subclinical atherosclerosis are a priority for primary prevention. This study takes a practical approach to answering a challenge commonly faced by primary care practitioners: in patients with no known CVD, how can individuals likely to have subclinical atherosclerosis be easily identified using existing clinical data and/or information provided by the patient?
Methods: Using NHANES (1999-2004), 6091 men and women aged ≥40 years without any CVD comprised the primary prevention population for this study. Subclinical atherosclerosis was determined via ankle-brachial index (ABI) using established cutoffs (subclinical atherosclerosis defined as ABI (0.91-0.99); normal defined as ABI (1.00-1.30)). Three common scores were calculated: the Framingham Risk Score (FRS), the Metabolic Syndrome (MetS), and the Cardiovascular Health Index (CVHI). Logistic regression analysis assessed the association between these scores and subclinical atherosclerosis. The sensitively and specificity of these scores in identifying subclinical atherosclerosis was determined.
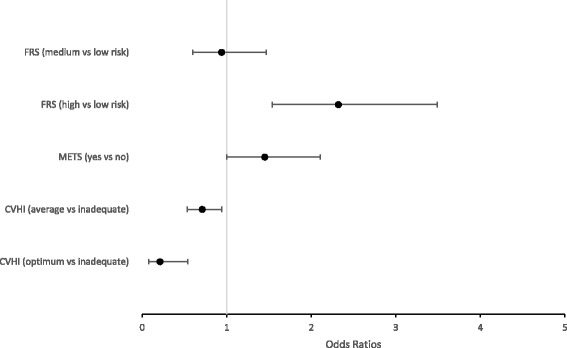
Results: In eligible participants, 3.8% had subclinical atherosclerosis. Optimum and average CVHI was associated with decreased odds for subclinical atherosclerosis. High, but not intermediate-risk, FRS was associated with increased odds for subclinical atherosclerosis. MetS was not associated with subclinical atherosclerosis. Of the 3 scores, CVHI was the most sensitive in identifying subclinical atherosclerosis and had the lowest number of missed cases. The FRS was the most specific but least sensitive of the 3 scores, and had almost 10-fold more missed cases vs. the CVHI. The MetS had "middle" sensitivity and specificity, and 10-fold more missed cases vs. the CVHI.
Conclusions: Results from this study suggest that routine administration of the CVHI in a primary prevention population would yield the benefits of identifying patients with existing subclinical CVD not identified through traditional CVD risk factors or scores, and bring physical activity and nutrition to the forefront of provider-patient discussions about lifestyle factors critical to maintaining and prolonging cardiovascular health.
Keywords: Ankle brachial index; Cardiovascular Health Index; Cardiovascular disease prevention; Cardiovascular risk factors; Framingham Risk Score; Metabolic syndrome; NHANES; Primary prevention; Subclinical atherosclerosis.
Conflict of interest statement
Ethics approval and consent to participate
All data used for this study were from obtained from publicly available datasets. This study was approved as exempt by the University of Western Ontario Research Ethics Board and as non-human subjects research by the West Virginia University Institutional Review Board.
Consent for publication
N/A
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
The Relationship between Cardiovascular Risk Scores and Several Markers of Subclinical Atherosclerosis in an Asymptomatic Population.J Clin Med. 2021 Mar 1;10(5):955. doi: 10.3390/jcm10050955. J Clin Med. 2021. PMID: 33804436 Free PMC article.
-
Subclinical cardiovascular disease assessment and its relationship with cardiovascular risk SCORE in a healthy adult population: A cross-sectional community-based study.Clin Investig Arterioscler. 2017 May-Jun;29(3):111-119. doi: 10.1016/j.arteri.2016.10.004. Epub 2017 Apr 1. Clin Investig Arterioscler. 2017. PMID: 28377040 English, Spanish.
-
Dietary patterns, smoking, and subclinical heart disease in women: opportunities for primary prevention from the Framingham Nutrition Studies.J Am Diet Assoc. 2004 Feb;104(2):208-14. doi: 10.1016/j.jada.2003.11.007. J Am Diet Assoc. 2004. PMID: 14760568
-
Primary Prevention of Subclinical Atherosclerosis in Young Adults: JACC Review Topic of the Week.J Am Coll Cardiol. 2023 Nov 28;82(22):2152-2162. doi: 10.1016/j.jacc.2023.09.817. J Am Coll Cardiol. 2023. PMID: 37993206 Review.
-
The Effect of Vitamin Supplementation on Subclinical Atherosclerosis in Patients without Manifest Cardiovascular Diseases: Never-ending Hope or Underestimated Effect?Molecules. 2020 Apr 9;25(7):1717. doi: 10.3390/molecules25071717. Molecules. 2020. PMID: 32283588 Free PMC article. Review.
Cited by
-
Female-specific risk factors of parity and menopause age and risk of carotid plaque: the multi-ethnic study of atherosclerosis.Am J Cardiovasc Dis. 2023 Aug 15;13(4):222-234. eCollection 2023. Am J Cardiovasc Dis. 2023. PMID: 37736349 Free PMC article.
-
Association between Alcohol Intake and Arterial Stiffness in Healthy Adults: A Systematic Review.Nutrients. 2022 Mar 12;14(6):1207. doi: 10.3390/nu14061207. Nutrients. 2022. PMID: 35334865 Free PMC article.
-
The Relationship between Cardiovascular Risk Scores and Several Markers of Subclinical Atherosclerosis in an Asymptomatic Population.J Clin Med. 2021 Mar 1;10(5):955. doi: 10.3390/jcm10050955. J Clin Med. 2021. PMID: 33804436 Free PMC article.
-
Poor cardiovascular health is associated with subclinical atherosclerosis in apparently healthy sub-Saharan African populations: an H3Africa AWI-Gen study.BMC Med. 2021 Feb 10;19(1):30. doi: 10.1186/s12916-021-01909-6. BMC Med. 2021. PMID: 33563289 Free PMC article.
-
Clinical significance of subclinical atherosclerosis in retinal vein occlusion.Sci Rep. 2021 Jun 7;11(1):11905. doi: 10.1038/s41598-021-91401-1. Sci Rep. 2021. PMID: 34099806 Free PMC article.
References
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–45. doi: 10.1161/01.cir.0000437738.63853.7a. - DOI - PubMed
-
- Goff DC, Jr, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S49–S73. doi: 10.1161/01.cir.0000437741.48606.98. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
