

Capture of intraocular lens optic by residual capsular opening in secondary implantation: long-term follow-up
- PMID: 29609595
- PMCID: PMC5880010
- DOI: 10.1186/s12886-018-0741-2
Capture of intraocular lens optic by residual capsular opening in secondary implantation: long-term follow-up
Abstract
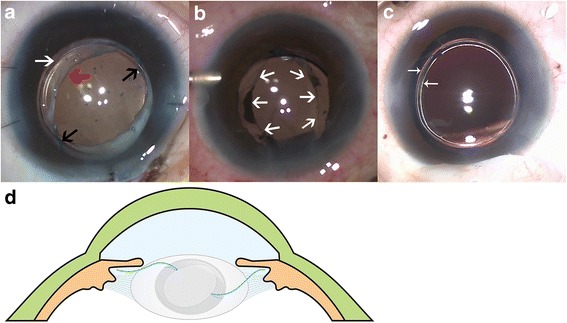
Background: To introduce a novel surgical technique for optic capture by residual capsular opening in secondary intraocular lens (IOL) implantation and to report the outcomes of a long follow-up.
Methods: Twenty patients (20 eyes) who had received secondary IOL implantation with the optic capture technique were retrospectively reviewed. We used the residual capsular opening for capturing the optic and inserted the haptics in the sulcus during surgery. Baseline clinical characteristics and surgical outcomes, including best-corrected visual acuity (BCVA), refractive status, and IOL position were recorded. The postoperative location and stability of IOL were evaluated using the ultrasound biomicroscopy.
Results: Optic capture technique was successfully performed in all cases, including 5 cases with large area of posterior capsular opacity, 6 cases with posterior capsular tear or rupture,and 9 cases with adhesive capsules. BCVA improved from 0.60 logMAR at baseline to 0.36 logMAR at the last follow-up (P < 0.001). Spherical equivalent changed from 10.67 ± 4.59 D at baseline to 0.12 ± 1.35 D at 6 months postoperatively (P < 0.001). Centered IOLs were observed in all cases and remained captured through residual capsular opening in 19 (95%) eyes at the last follow-up. In one case, the captured optic of IOL slid into ciliary sulcus at 7 months postoperatively. No other postoperative complications were observed in any cases.
Conclusions: This optic capture technique by using residual capsule opening is an efficacious and safe technique and can achieve IOL stability in the long follow-up.
Keywords: Dislocation; Intraocular lens; Optic capture; Secondary IOL implantation.
Conflict of interest statement
Ethics approval and consent to participate
This study adhered to the tenets of the Declaration of Helsinki and was approved by institution review board of Xinhua hospital affiliated to medical college, Shanghai Jiaotong University. The written informed consent to participate was obtained from each patient or his or her parent(s)/ legal guardian(s).
Consent for publication
The written consent for publication of the individual details and images was obtained from each patient. For patients under 18-year old, the written consent was obtained from his/her parent (s) or legal guardian(s). The written consent was obtained from the patient’s parents whose images were shown in Fig. 4.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



Similar articles
-
Posterior optic capture for repositioning of dislocated three-piece intraocular lens: a single center retrospective study.BMC Ophthalmol. 2025 May 23;25(1):308. doi: 10.1186/s12886-025-04147-z. BMC Ophthalmol. 2025. PMID: 40410726 Free PMC article.
-
Intraocular lens optic capture.J Cataract Refract Surg. 2004 Jan;30(1):200-6. doi: 10.1016/j.jcrs.2003.11.035. J Cataract Refract Surg. 2004. PMID: 14967291 Review.
-
Long-term outcomes of ciliary sulcus versus capsular bag fixation of intraocular lenses in children: An ultrasound biomicroscopy study.PLoS One. 2017 Mar 16;12(3):e0172979. doi: 10.1371/journal.pone.0172979. eCollection 2017. PLoS One. 2017. PMID: 28301497 Free PMC article.
-
Posterior vertical capsulotomy with optic entrapment of the intraocular lens in congenital cataracts--prevention of capsule opacification.J Cataract Refract Surg. 2005 May;31(5):886-94. doi: 10.1016/j.jcrs.2004.08.055. J Cataract Refract Surg. 2005. PMID: 15975452
-
[Sutureless scleral intraocular lens fixation: report of nine cases and literature review].J Fr Ophtalmol. 2013 Oct;36(8):658-68. doi: 10.1016/j.jfo.2012.09.009. Epub 2013 Jul 25. J Fr Ophtalmol. 2013. PMID: 23891322 Review. French.
Cited by
-
Posterior optic capture for repositioning of dislocated three-piece intraocular lens: a single center retrospective study.BMC Ophthalmol. 2025 May 23;25(1):308. doi: 10.1186/s12886-025-04147-z. BMC Ophthalmol. 2025. PMID: 40410726 Free PMC article.
-
Intraocular Lens Elongation Technique with Haptic Modification for Sulcus Implantation.Turk J Ophthalmol. 2022 Aug 25;52(4):223-227. doi: 10.4274/tjo.galenos.2021.38275. Turk J Ophthalmol. 2022. PMID: 36016578 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
