

Clinical features of children with enthesitis-related juvenile idiopathic arthritis / juvenile spondyloarthritis followed in a French tertiary care pediatric rheumatology centre
- PMID: 29609643
- PMCID: PMC5879929
- DOI: 10.1186/s12969-018-0238-9
Clinical features of children with enthesitis-related juvenile idiopathic arthritis / juvenile spondyloarthritis followed in a French tertiary care pediatric rheumatology centre
Abstract
Background: Childhood-onset spondyloarthropathies usually start with enthesitis and peripheral arthritis. However, axial disease may develop afterward. Patients are most often classified, following revised (Edmonton 2011) ILAR criteria, as enthesitis-related arthritis, psoriatic arthritis, or unclassified juvenile idiopathic arthritis, particularly in cases of psoriasis in the patient or a first-degree relative. In adults, peripheral spondyloarthritis is classified by ASAS criteria.
Methods: We retrospectively studied patients with childhood-onset spondyloarthropathies followed for more than one year in our referral centre. We did not exclude patients with a personal or familial history of psoriasis.
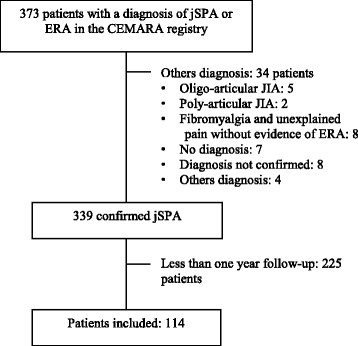
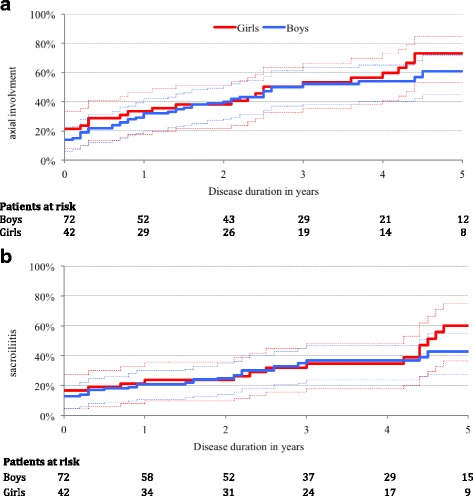
Results: We included 114 patients followed between January 2008 and December 2015 for a median of 2.5 years (IQR = 2.3). Sixty-nine per-cent of patients fulfilled the revised ILAR classification criteria for enthesitis-related arthritis, and 92% the ASAS criteria for peripheral spondyolarthritis (p < 0.001). Axial disease and sacroiliitis were rare at disease onset. However, they appeared during follow-up in 63% and 47% of cases respectively, after a median disease duration of 2.6 (IC 95% [2.2-4.4]) and 5.3 years (IC 95% [4.1-7.7]), respectively. Multivariable analysis showed that familial history of spondyloarthritis was associated with the presence of sacroiliitis and active disease at the latest follow-up (OR = 3.61 [1.5-8.7], p < 0.01 and 2.98 [1.2-7.3], p = 0.02, respectively).
Conclusion: Axial involvement developed in most patients within five years. Revised Edmonton criteria were less sensitive than ASAS criteria to classify patients as having childhood-onset spondyloarthropathies. The main risk factor for both sacroiliitis and persistent active disease was a familial history of spondyloarthritis.
Keywords: Anti-TNF treatment; Classification criteria; Enthesitis related arthritis; Juvenile idiopathic arthritis; Juvenile spondyloarthritis; Prognostic factor.
Conflict of interest statement
Ethics approval and consent to participate
The CEMARA system has authorisation from the French National Committee on Informatics and Liberty (CNIL). According to the French legislation, patients and parents were informed, but no informed consent form was required for a retrospective analysis.
Consent for publication
Not applicable
Competing interests
Maxime Goirand: invited to an international congress by Novartis. Richard Mouy, Brigitte Bader-Meunier, and Pierre Quartier: investigators in clinical trials on ERA for Abbvie and Pfizer. Pierre Quartier: consultant for Abbvie, speaker and congress invitations by Abbvie and Pfizer.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31:390–392. - PubMed
-
- Burgos-Vargas R. The assessment of the spondyloarthritis international society concept and criteria for the classification of axial spondyloarthritis and peripheral spondyloarthritis: a critical appraisal for the pediatric rheumatologist. Pediatr Rheum Online J. 2012;10:14. doi: 10.1186/1546-0096-10-14. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
