

Perceived Treatment Status of Fluctuations in Parkinson Disease Impacts Suicidality
- PMID: 29609901
- PMCID: PMC5993611
- DOI: 10.1016/j.jagp.2018.01.005
Perceived Treatment Status of Fluctuations in Parkinson Disease Impacts Suicidality
Abstract
Objective: On/off motor fluctuations in Parkinson disease (PD) can be associated with extreme mood fluctuations and severe dysphoria. The impact of these affective symptoms may be overlooked in the treatment of motor fluctuations. Our goal was to examine the relationship between motor fluctuations, their treatment status, and suicidality in PD participants.
Methods: We analyzed data from the Methods of Optimal Depression Detection in Parkinson's Disease (MOOD-PD) study of 223 individuals with PD. Suicidality was measured using items from four depression scales: Hamilton Depression Rating Scale (HAM-D-17); Montgomery-Åsberg Depression Rating Scale (MADRS); Inventory for Depressive Symptomatology (IDS-C); and the self-rated Beck Depression Inventory (BDI). Multivariable Poisson regression analyses tested whether self-reported motor fluctuations and their treatment status were associated with suicidality while controlling for recognized risk factors.
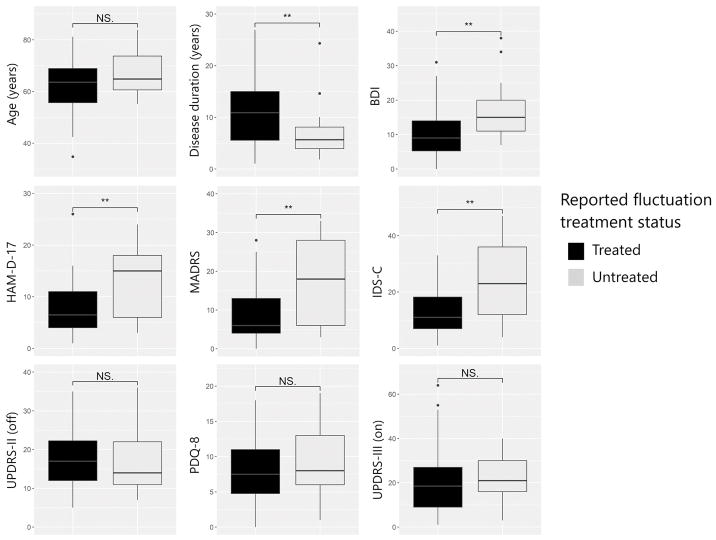
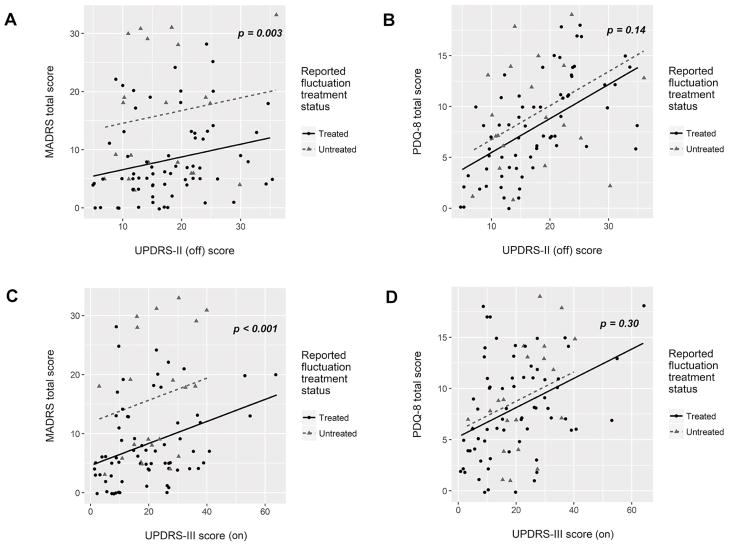
Results: Thirty-seven participants (16.6%) self-reported suicidality and 89 (39.5%) self-reported motor fluctuations, of whom 21 (23.6%) perceived their fluctuations as untreated. Participants reporting untreated motor fluctuations more frequently had a current depressive disorder (p < 0.001) and endorsed suicidality (p = 0.006) than participants with treated or no fluctuations. They also had significantly higher total scores on the HAM-D-17, MADRS, IDS-C, and BDI depression scales (p < 0.001 for each). Regression analyses showed significant associations between untreated motor fluctuations and higher scores on suicide questions extracted from the HAM-D-17, MADRS, and IDS-C (p < 0.01 for each).
Conclusions: PD patients with untreated motor fluctuations are at increased risk for suicidal thoughts and should be monitored for mood changes as treatment is adapted.
Keywords: Parkinson disease; depression; fluctuations; suicide.
Copyright © 2018 American Association for Geriatric Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
A comparison of nine scales to detect depression in Parkinson disease: which scale to use?Neurology. 2012 Mar 27;78(13):998-1006. doi: 10.1212/WNL.0b013e31824d587f. Epub 2012 Mar 14. Neurology. 2012. PMID: 22422897 Free PMC article. Clinical Trial.
-
The assessment of depression in Parkinson's disease.Eur J Neurol. 2008 May;15(5):487-92. doi: 10.1111/j.1468-1331.2008.02101.x. Epub 2008 Mar 18. Eur J Neurol. 2008. PMID: 18355310
-
Suicidal risk and demoralization in Parkinson disease.J Neurol. 2020 Apr;267(4):966-974. doi: 10.1007/s00415-019-09632-2. Epub 2019 Dec 4. J Neurol. 2020. PMID: 31802218
-
Depression rating scales in Parkinson's disease: A critical review updating recent literature.J Affect Disord. 2015 Sep 15;184:216-24. doi: 10.1016/j.jad.2015.05.059. Epub 2015 Jun 10. J Affect Disord. 2015. PMID: 26114228 Review.
-
Depression in Parkinson's disease: diagnosis and treatment.Arq Neuropsiquiatr. 2012 Aug;70(8):617-20. doi: 10.1590/s0004-282x2012000800011. Arq Neuropsiquiatr. 2012. PMID: 22899034 Review.
References
-
- Chaudhuri KR, Healy DG, Schapira AHV. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006;5:235–245. - PubMed
-
- Remy P, Doder M, Lees A, Turjanski N, Brooks D. Depression in Parkinson’s disease: loss of dopamine and noradrenaline innervation in the limbic system. Brain. 2005;128:1314–1322. - PubMed
-
- Reijnders J, Ehrt U, Weber W, Aarsland D, Leentjens A. A systematic review of prevalence studies of depression in Parkinson’s disease. Mov Disord. 2008;23:183–9. quiz 313. - PubMed
-
- Kostić VS, Pekmezović T, Tomić A, et al. Suicide and suicidal ideation in Parkinson’s disease. J Neurol Sci. 2009;289:40–43. - PubMed
-
- Leentjens AFG, Marinus J, Van Hilten JJ, Lousberg R, Verhey FRJ. The contribution of somatic symptoms to the diagnosis of depressive disorder in Parkinson’s disease: a discriminant analytic approach. J Neuropsychiatry Clin Neurosci. 2003;15:74–77. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
