

Use of an Assistant Surgeon Does not Mitigate the Effect of Lead Surgeon Volume on Outcomes Following Open Repair of Intact Abdominal Aortic Aneurysms
- PMID: 29609964
- PMCID: PMC5940521
- DOI: 10.1016/j.ejvs.2018.02.026
Use of an Assistant Surgeon Does not Mitigate the Effect of Lead Surgeon Volume on Outcomes Following Open Repair of Intact Abdominal Aortic Aneurysms
Abstract
Objective/background: While higher lead surgeon volume has been associated with lower mortality following open abdominal aortic aneurysm (AAA) repair, little is known about the impact of using an attending surgeon as assistant surgeon. The aim of this study was to determine whether the presence of an assistant surgeon, particularly a high volume assistant, mitigates the relationship between lead surgeon volume and outcomes.
Methods: All Medicare beneficiaries who underwent intact, open AAA repair between 2003 and 2008 were evaluated and nested regression models were constructed to evaluate the relationship between surgeon and assistant volume and peri-operative mortality, adjusting for comorbid conditions and hospital volume.
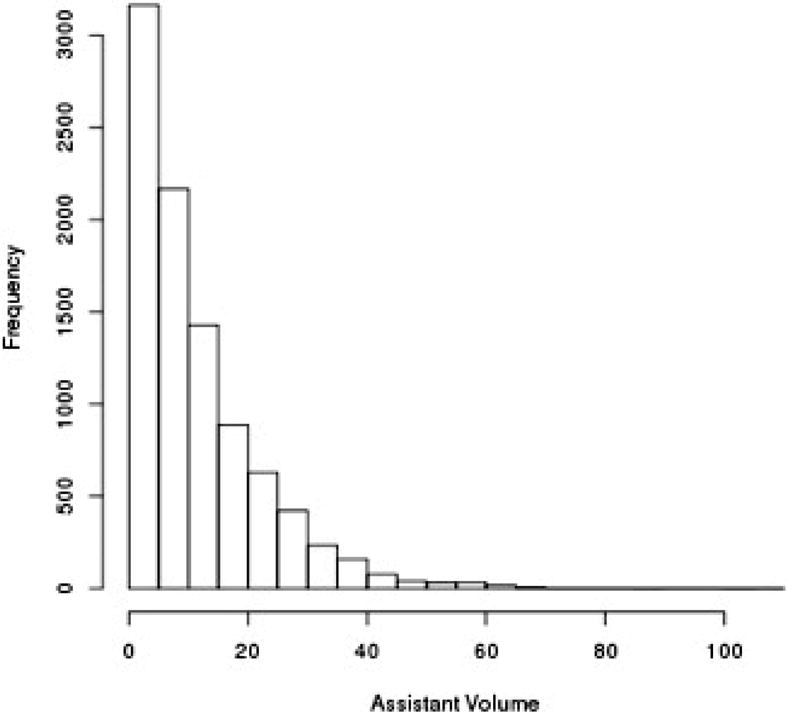
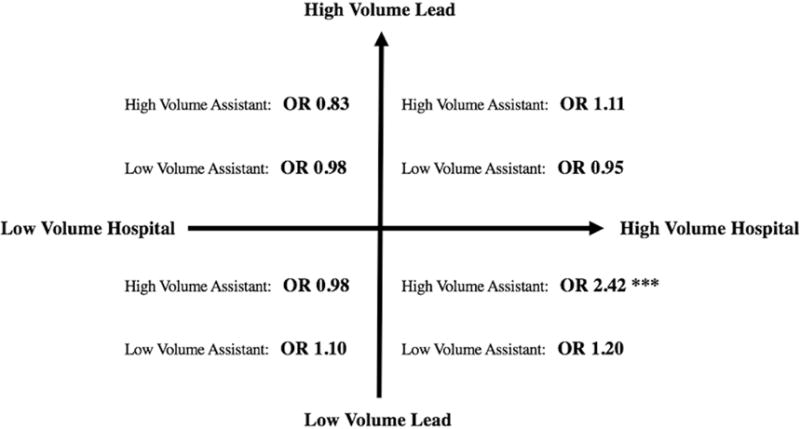
Results: In total 28,590 repairs were studied, of which 19,284 (67.5%) were performed by a single surgeon and 9306 (32.5%) included an assistant surgeon. Of cases with an assistant, 12.3% included a high volume assistant surgeon. Lower volume surgeons more frequently used an assistant (lead surgeon Q1 volume: 40%; Q2: 36%; Q3: 34%; Q4: 29%; Q5: 27% [p < .01]). In cases with no assistant, adjusted peri-operative mortality varied monotonically with surgeon volume (Q1: 4.7%; Q2: 4.4%; Q3: 4.1%; Q4: 3.3%; Q5: 3.2%). However, the use of a high or a low volume assistant surgeon, compared with no attending surgeon as assistant, was not associated with lower peri-operative mortality in any lead surgeon volume quintile, even among those operations performed by the lowest volume lead surgeons.
Conclusion: Employing an assistant surgeon does not improve outcomes amongst any quintile of volume of the lead surgeon. As surgeons perform fewer open AAA repairs in the modern era, these data imply that even the help of a high volume assistant surgeon may not mitigate the detrimental effect of a lower volume surgeon.
Keywords: AAA; Assistant; Open repair; Volume.
Copyright © 2018 European Society for Vascular Surgery. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
MLS is a consultant for Abbott, Medtronic, and Endologix.
Figures

Comment in
-
Do Many Hands Make Outcomes Better? Commentary on "Use of an Assistant Surgeon Does Not Mitigate the Effect of Lead Surgeon Volume on Outcomes Following Open Repair of Intact Abdominal Aneurysms".Eur J Vasc Endovasc Surg. 2018 May;55(5):720. doi: 10.1016/j.ejvs.2018.03.003. Epub 2018 Mar 27. Eur J Vasc Endovasc Surg. 2018. PMID: 29602621 No abstract available.
Similar articles
-
Higher surgeon annual volume, but not years of experience, is associated with reduced rates of postoperative complications and reoperations after open abdominal aortic aneurysm repair.J Vasc Surg. 2018 Jun;67(6):1717-1726.e5. doi: 10.1016/j.jvs.2017.10.050. Epub 2017 Dec 13. J Vasc Surg. 2018. PMID: 29248240
-
The Relationship Between Operative Volume and Peri-operative Mortality After Non-elective Aortic Aneurysm Repair in Australia.Eur J Vasc Endovasc Surg. 2020 Oct;60(4):519-530. doi: 10.1016/j.ejvs.2020.04.029. Epub 2020 Jul 2. Eur J Vasc Endovasc Surg. 2020. PMID: 32624387
-
Surgeon volume and established hospital perioperative mortality rate together predict for superior outcomes after open abdominal aortic aneurysm repair.J Vasc Surg. 2022 Feb;75(2):504-513.e3. doi: 10.1016/j.jvs.2021.08.077. Epub 2021 Sep 22. J Vasc Surg. 2022. PMID: 34560221
-
Comparison of endovascular and open surgical repairs for abdominal aortic aneurysm.Evid Rep Technol Assess (Full Rep). 2006 Aug;(144):1-113. Evid Rep Technol Assess (Full Rep). 2006. PMID: 17764213 Free PMC article. Review.
-
Provider volume and outcomes for abdominal aortic aneurysm repair, carotid endarterectomy, and lower extremity revascularization procedures.J Vasc Surg. 2007 Mar;45(3):615-26. doi: 10.1016/j.jvs.2006.11.019. J Vasc Surg. 2007. PMID: 17321352 Review.
Cited by
-
Effect of annualized surgeon volume on major surgical complications for abdominal and laparoscopic radical hysterectomy for cervical cancer in China, 2004-2016: a retrospective cohort study.BMC Womens Health. 2023 Feb 15;23(1):69. doi: 10.1186/s12905-023-02213-6. BMC Womens Health. 2023. PMID: 36793026 Free PMC article.
References
-
- Dimick JB, Cowan JA, Jr, Stanley JC, Henke PK, Pronovost PJ, Upchurch GR., Jr Surgeon specialty and provider volumes are related to outcome of intact abdominal aortic aneurysm repair in the United States. J Vasc Surg. 2003;38:739–44. - PubMed
-
- McPhee JT, Robinson WP, 3rd, Eslami MH, Arous EJ, Messina LM, Schanzer A. Surgeon case volume, not institution case volume, is the primary determinant of in-hospital mortality after elective open abdominal aortic aneurysm repair. J Vasc Surg. 2011;53:591–9.e2. - PubMed
-
- Holt PJ, Poloniecki JD, Gerrard D, Loftus IM, Thompson MM. Meta-analysis and systematic review of the relationship between volume and outcome in abdominal aortic aneurysm surgery. Br J Surg. 2007;94:395–403. - PubMed
-
- Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume and operative mortality in the United States. N Engl J Med. 2003;349:2117–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
