

Hypomagnesemia in critically ill patients
- PMID: 29610664
- PMCID: PMC5872533
- DOI: 10.1186/s40560-018-0291-y
Hypomagnesemia in critically ill patients
Abstract
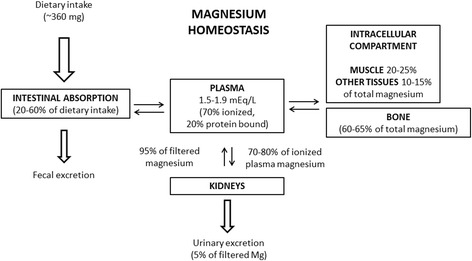
Background: Magnesium (Mg) is essential for life and plays a crucial role in several biochemical and physiological processes in the human body. Hypomagnesemia is common in all hospitalized patients, especially in critically ill patients with coexisting electrolyte abnormalities. Hypomagnesemia may cause severe and potential fatal complications if not timely diagnosed and properly treated, and associate with increased mortality.
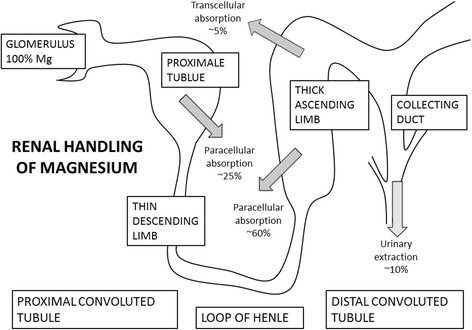
Main body: Mg deficiency in critically ill patients is mainly caused by gastrointestinal and/or renal disorders and may lead to secondary hypokalemia and hypocalcemia, and severe neuromuscular and cardiovascular clinical manifestations. Because of the physical distribution of Mg, there are no readily or easy methods to assess Mg status. However, serum Mg and the Mg tolerance test are most widely used. There are limited studies to guide intermittent therapy of Mg deficiency in critically ill patients, but some empirical guidelines exist. Further clinical trials and critical evaluation of empiric Mg replacement strategies is needed.
Conclusion: Patients at risk of Mg deficiency, with typical biochemical findings or clinical symptoms of hypomagnesemia, should be considered for treatment even with serum Mg within the normal range.
Keywords: Arrhythmia; Calcium; Critical illness; Intensive care unit; Magnesium; Potassium.
Conflict of interest statement
No approval is required.No consent is required.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Whang R, Oei TO, Aikawa JK, Watanabe A, Vannatta J, Fryer A, et al. Predictors of clinical hypomagnesemia. Hypokalemia, hypophosphatemia, hyponatremia, and hypocalcemia. Arch Intern Med. 1984;144:1794–1796. - PubMed
-
- Wong ET, Rude RK, Singer FR, Shaw ST., Jr A high prevalence of hypomagnesemia and hypermagnesemia in hospitalized patients. Am J Clin Pathol. 1983;79:348–352. - PubMed
-
- Hayes JP, Ryan MF, Brazil N, Riordan TO, Walsh JB, Coakley D. Serum hypomagnesaemia in an elderly day-hospital population. Ir Med J. 1989;82:117–119. - PubMed
-
- Reinhart RA, Desbiens NA. Hypomagnesemia in patients entering the ICU. Crit Care Med. 1985;13:506–507. - PubMed
-
- Ryzen E, Wagers PW, Singer FR, Rude RK. Magnesium deficiency in a medical ICU population. Crit Care Med. 1985;13:19–21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
