

Effect of Central Line Bundle Compliance on Central Line-Associated Bloodstream Infections
- PMID: 29611399
- PMCID: PMC5889989
- DOI: 10.3349/ymj.2018.59.3.376
Effect of Central Line Bundle Compliance on Central Line-Associated Bloodstream Infections
Abstract
Purpose: The present study aimed to evaluate the effect of central line (CL) bundle compliance on central line-associated bloodstream infections (CLABSIs) in different departments of the same hospital, including the intensive care unit (ICU) and other departments.
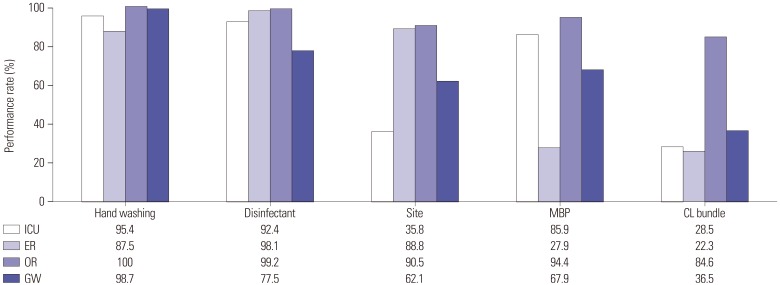
Materials and methods: The four components of the CL bundle were hand hygiene, use of maximal sterile barrier precautions, chlorhexidine use, and selection of an appropriate site for venous access. Compliance of the CL bundle and CLABSIs were measured for every department [emergency room (ER), ICU, general ward (GW), and operating room (OR)]. A total of 1672 patients were included over 3 years (August 2013 through July 2016).
Results: A total of 29 CLABSI episodes (1.73%) were identified, and only 53.7% of the patients completed CL bundles. The performance rates of all components of the CL bundle were 22.3%, 28.5%, 36.5%, and 84.6% for the ER, ICU, GW, and OR, respectively. The highest CLABSI rate was observed in patients of the ICU, for whom all components were not performed perfectly. Conversely, the lowest CLABSI rate was observed for patients of GWs, for whom all components were performed. Among individual components, femoral insertion site [relative risk (RR), 2.26; 95% confidence interval (CI), 1.09-4.68], not using a full body drape (RR, 3.55; 95% CI, 1.44-8.71), and not performing all CL bundle components (RR, 2.79; 95% CI, 1.19-6.54) were significant variables associated with CLABSIs.
Conclusion: This study provides direct evidence that completing all CL bundle components perfectly is essential for preventing CLABSIs. Customized education should be provided, according to specific weaknesses of bundle performance.
Keywords: Central venous catheter; catheter-associated infection; central line bundle.
© Copyright: Yonsei University College of Medicine 2018.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Stevens V, Geiger K, Concannon C, Nelson RE, Brown J, Dumyati G. Inpatient costs, mortality and 30-day re-admission in patients with central-line-associated bloodstream infections. Clin Microbiol Infect. 2014;20:O318–O324. - PubMed
-
- Ziegler MJ, Pellegrini DC, Safdar N. Attributable mortality of central line associated bloodstream infection: systematic review and meta-analysis. Infection. 2015;43:29–36. - PubMed
-
- Al-Rawajfah OM, Hewitt JB, Stetzer F, Cheema J. Length of stay and charges associated with health care-acquired bloodstream infections. Am J Infect Control. 2012;40:227–232. - PubMed
-
- Umscheid CA, Mitchell MD, Doshi JA, Agarwal R, Williams K, Brennan PJ. Estimating the proportion of healthcare-associated infections that are reasonably preventable and the related mortality and costs. Infect Control Hosp Epidemiol. 2011;32:101–114. - PubMed
-
- Marschall J, Mermel LA, Fakih M, Hadaway L, Kallen A, O'Grady NP, et al. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(Suppl 2):S89–S107. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
