

Association of Solid Fuel Use With Risk of Cardiovascular and All-Cause Mortality in Rural China
- PMID: 29614179
- PMCID: PMC5933384
- DOI: 10.1001/jama.2018.2151
Association of Solid Fuel Use With Risk of Cardiovascular and All-Cause Mortality in Rural China
Abstract
Importance: When combusted indoors, solid fuels generate a large amount of pollutants such as fine particulate matter.
Objective: To assess the associations of solid fuel use for cooking and heating with cardiovascular and all-cause mortality.
Design, setting, and participants: This nationwide prospective cohort study recruited participants from 5 rural areas across China between June 2004 and July 2008; mortality follow-up was until January 1, 2014. A total of 271 217 adults without a self-reported history of physician-diagnosed cardiovascular disease at baseline were included, with a random subset (n = 10 892) participating in a resurvey after a mean interval of 2.7 years.
Exposures: Self-reported primary cooking and heating fuels (solid: coal, wood, or charcoal; clean: gas, electricity, or central heating), switching of fuel type before baseline, and use of ventilated cookstoves.
Main outcomes and measures: Death from cardiovascular and all causes, collected through established death registries.
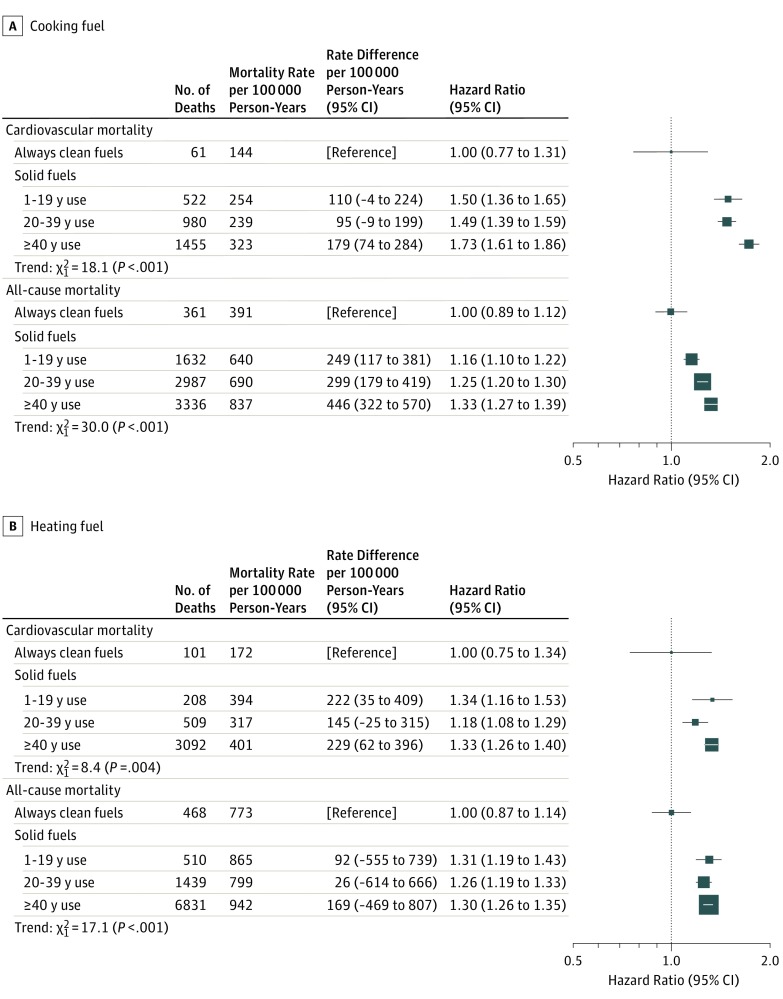
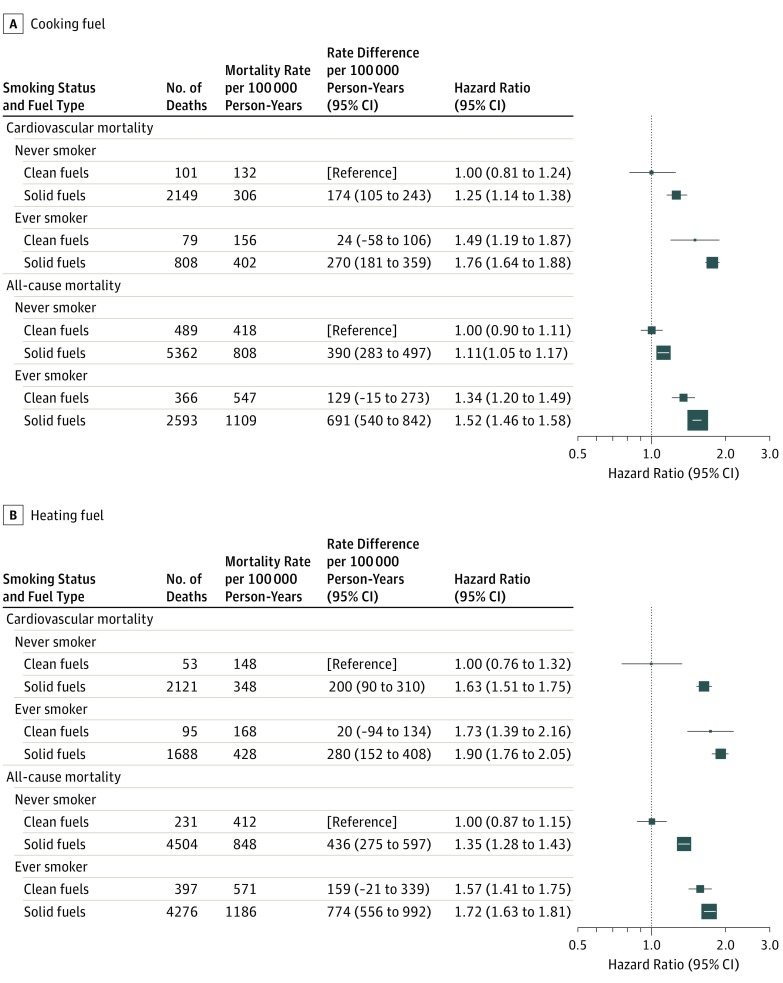
Results: Among the 271 217 participants, the mean (SD) age was 51.0 (10.2) years, and 59% (n = 158 914) were women. A total of 66% (n = 179 952) of the participants reported regular cooking (at least weekly) and 60% (n = 163 882) reported winter heating, of whom 84% (n = 150 992) and 90% (n = 147 272) used solid fuels, respectively. There were 15 468 deaths, including 5519 from cardiovascular causes, documented during a mean (SD) of 7.2 (1.4) years of follow-up. Use of solid fuels for cooking was associated with greater risk of cardiovascular mortality (absolute rate difference [ARD] per 100 000 person-years, 135 [95% CI, 77-193]; hazard ratio [HR], 1.20 [95% CI, 1.02-1.41]) and all-cause mortality (ARD, 338 [95% CI, 249-427]; HR, 1.11 [95% CI, 1.03-1.20]). Use of solid fuels for heating was also associated with greater risk of cardiovascular mortality (ARD, 175 [95% CI, 118-231]; HR, 1.29 [95% CI, 1.06-1.55]) and all-cause mortality (ARD, 392 [95% CI, 297-487]; HR, 1.14 [95% CI, 1.03-1.26]). Compared with persistent solid fuel users, participants who reported having previously switched from solid to clean fuels for cooking had a lower risk of cardiovascular mortality (ARD, 138 [95% CI, 71-205]; HR, 0.83 [95% CI, 0.69-0.99]) and all-cause mortality (ARD, 407 [95% CI, 317-497]; HR, 0.87 [95% CI, 0.79-0.95]), while for heating, the ARDs were 193 (95% CI, 128-258) and 492 (95% CI, 383-601), and the HRs were 0.57 (95% CI, 0.42-0.77) and 0.67 (95% CI, 0.57-0.79), respectively. Among solid fuel users, use of ventilated cookstoves was also associated with lower risk of cardiovascular mortality (ARD, 33 [95% CI, -9 to 75]; HR, 0.89 [95% CI, 0.80-0.99]) and all-cause mortality (ARD, 87 [95% CI, 20-153]; HR, 0.91 [95% CI, 0.85-0.96]).
Conclusions and relevance: In rural China, solid fuel use for cooking and heating was associated with higher risks of cardiovascular and all-cause mortality. These risks may be lower among those who had previously switched to clean fuels and those who used ventilation.
Conflict of interest statement
Figures
References
-
- International Energy Agency World Energy Outlook 2016. Paris, France: International Energy Agency; 2016.
-
- GBD 2016 Risk Factors Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345-1422. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
