

A novel citrate-based protocol versus heparin anticoagulation for sustained low-efficiency dialysis in the ICU: safety, efficacy, and cost
- PMID: 29614970
- PMCID: PMC5883400
- DOI: 10.1186/s12882-018-0879-4
A novel citrate-based protocol versus heparin anticoagulation for sustained low-efficiency dialysis in the ICU: safety, efficacy, and cost
Abstract
Background: The high cost, complexity of the available protocols, and metabolic complications are the major barriers that impede the clinical utilization of regional citrate anticoagulation (RCA) for sustained low efficiency dialysis (SLED) in critically ill patients. By comparing a novel protocol for SLED using 30% citrate solution with common protocol using unfractionated heparin, this study aimed to provide new insights for clinical applications of RCA.
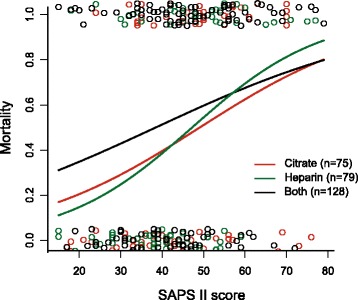
Methods: In this retrospective study, a total of 282 critically ill patients who underwent SLED with citrate and/or heparin anticoagulation in six adult ICUs were enrolled. These patients were divided into three groups based on the anticoagulation regimens they had received during the treatment in ICU: Group 1 (Citrate) had only received treatment with citrate anticoagulation (n=75); Group 2 (Heparin) only with heparin anticoagulation (n=79); and Group 3 (Both) with both citrate and heparin anticoagulation (n=128). We compared the mortality, metabolic complications as well as cost among these groups using different anticoagulation regimens.
Results: The in-hospital mortality did not significantly differ among groups (p> 0.1). However, three patients in heparin group suffered from severe bleeding which led to death, while none in citrate group. Overall, 976 SLED sessions with heparin anticoagulation and 808 with citrate were analyzed. The incidence of extracorporeal circuit clotting was significantly less in citrate (5%), as compared to that in heparin (10%) (p< 0.001). Metabolic complications and hypotension which led to interruption of SLED occurred more frequently, though not significantly, in citrate (p= 0.06, p= 0.23). Furthermore, with 30% citrate solution, the cost of anticoagulant was reduced by 70% in comparison to previously reported protocol using Acid Citrate Dextrose solution A (ACD-A).
Conclusions: Our results indicated that anticoagulation regimens for SLED did not significantly affect the mortality of patients. Citrate anticoagulation was superior to heparin in preventing severe bleeding and circuit clotting. The protocol adopted in this study using 30% citrate solution was safe as well as efficacious. In the meantime, it was much more cost-efficient than other citrate-based protocol.
Keywords: Critically ill patients; Regional citrate anticoagulation; Sustained low-efficiency dialysis.
Conflict of interest statement
Ethics approval and consent to participate
This study was carried out in accordance with the Declaration of Helsinki, and was approved by the institutional ethical review boards of the University Hospital rechts der Isar, Technical University Munich (213/16 S). All necessary written consent was obtained from the patients at the admission to the hospital. If the patients were incapable of providing consent due to an acute or chronic illness, written consent was obtained from legal guardian.
Consent for publication
Not applicable
Competing interests
All authors have read and approved the submission. None of the authors received financial support or funding for these investigations. The authors declare that they have no competing financial interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Safety of regional citrate anticoagulation for continuous sustained low efficiency dialysis (C-SLED) in critically ill patients.Ren Fail. 2005;27(5):541-5. doi: 10.1080/08860220500198748. Ren Fail. 2005. PMID: 16152991
-
Sustained Low-Efficiency Dialysis (SLED) with Regional Citrate Anticoagulation (RCA) and new dialysis equipment: a prospective study with serum citrate measurements and electrolyte monitoring.J Nephrol. 2025 Mar;38(2):473-480. doi: 10.1007/s40620-024-02201-5. Epub 2025 Feb 1. J Nephrol. 2025. PMID: 39891841
-
A Randomized Controlled Trial of Regional Citrate Versus Regional Heparin Anticoagulation for Continuous Renal Replacement Therapy in Critically Ill Adults.Crit Care Med. 2015 Aug;43(8):1622-9. doi: 10.1097/CCM.0000000000001004. Crit Care Med. 2015. PMID: 25853591 Clinical Trial.
-
Automated regional citrate anticoagulation: technological barriers and possible solutions.Blood Purif. 2010;29(2):204-9. doi: 10.1159/000245648. Epub 2010 Jan 8. Blood Purif. 2010. PMID: 20093828 Review.
-
Renal replacement therapy and anticoagulation.Best Pract Res Clin Anaesthesiol. 2017 Sep;31(3):387-401. doi: 10.1016/j.bpa.2017.08.005. Epub 2017 Aug 24. Best Pract Res Clin Anaesthesiol. 2017. PMID: 29248145 Review.
Cited by
-
Quality indicators in prolonged hemodialysis with regional citrate anticoagulation with the genius system: retrospective cohort of critical patients with acute kidney injury.BMC Nephrol. 2023 Nov 30;24(1):353. doi: 10.1186/s12882-023-03342-8. BMC Nephrol. 2023. PMID: 38036951 Free PMC article.
-
Care of the chronic dialysis patient in the intensive care unit: a state-of-the-art review.Crit Care Sci. 2025 Feb 24;37:e20250130. doi: 10.62675/2965-2774.20250130. eCollection 2025. Crit Care Sci. 2025. PMID: 40008694 Free PMC article. Review.
-
Regional citrate anticoagulation (RCA) in critically ill patients undergoing renal replacement therapy (RRT): expert opinion from the SIAARTI-SIN joint commission.J Anesth Analg Crit Care. 2023 Mar 31;3(1):7. doi: 10.1186/s44158-023-00091-w. J Anesth Analg Crit Care. 2023. PMID: 37386664 Free PMC article. Review.
-
Archetypal sustained low-efficiency daily diafiltration (SLEDD-f) for critically ill patients requiring kidney replacement therapy: towards an adequate therapy.J Nephrol. 2023 Sep;36(7):1789-1804. doi: 10.1007/s40620-023-01665-1. Epub 2023 Jun 21. J Nephrol. 2023. PMID: 37341966 Review.
-
Segmental citrate anticoagulation for double-filtration plasmapheresis: A case report and literature review.Med Int (Lond). 2022 May 31;2(3):18. doi: 10.3892/mi.2022.43. eCollection 2022 May-Jun. Med Int (Lond). 2022. PMID: 36698504 Free PMC article.
References
-
- Faulhaber-Walter R, Hafer C, Jahr N, Vahlbruch J, Hoy L, Haller H, Fliser D, Kielstein JT. The Hannover dialysis outcome study: comparison of standard versus intensified extended dialysis for treatment of patients with acute kidney injury in the intensive care unit. Nephrol Dial Transplant. 2009;24(7):2179–2186. doi: 10.1093/ndt/gfp035. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
