

Comparison of lateral entry with crossed entry pinning for pediatric supracondylar humeral fractures: a meta-analysis
- PMID: 29615086
- PMCID: PMC5883290
- DOI: 10.1186/s13018-018-0768-3
Comparison of lateral entry with crossed entry pinning for pediatric supracondylar humeral fractures: a meta-analysis
Abstract
Background: The standard treatment for severe displaced pediatric supracondylar humeral fracture (SCHF) is closed reduction and percutaneous pin fixation. However, controversy persists concerning the optimal pin fixation technique. The purpose of this study was to compare the safety and efficacy on the configuration of lateral entry only with crossed entry pin fixation for SCHF, including Gartland type II and type III fractures in children.
Methods: Published literatures, including retrospective studies, prospective studies, and randomized controlled trials, presenting the probability of poor functional consequence of elbow and/or loss of reduction and/or iatrogenic ulnar nerve injury and/or superficial infection and/or cubitus varus were included. Statistical analysis was performed with the Review Manager 5.3 software.
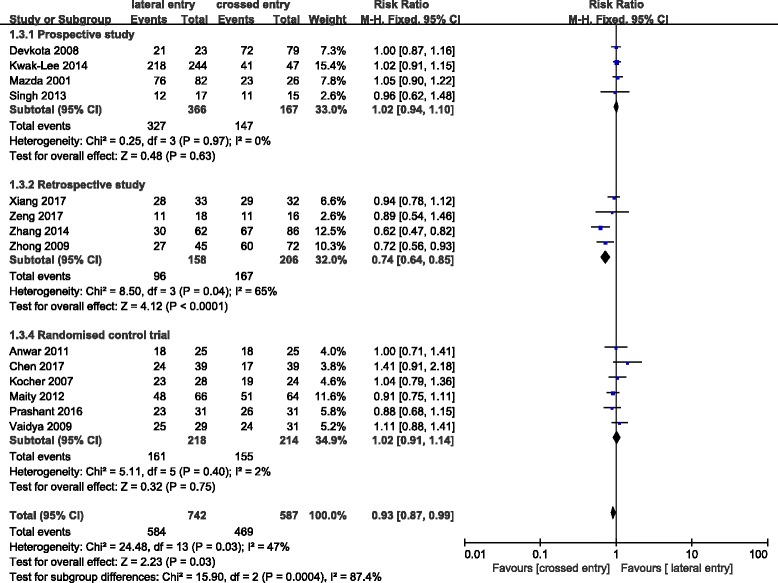
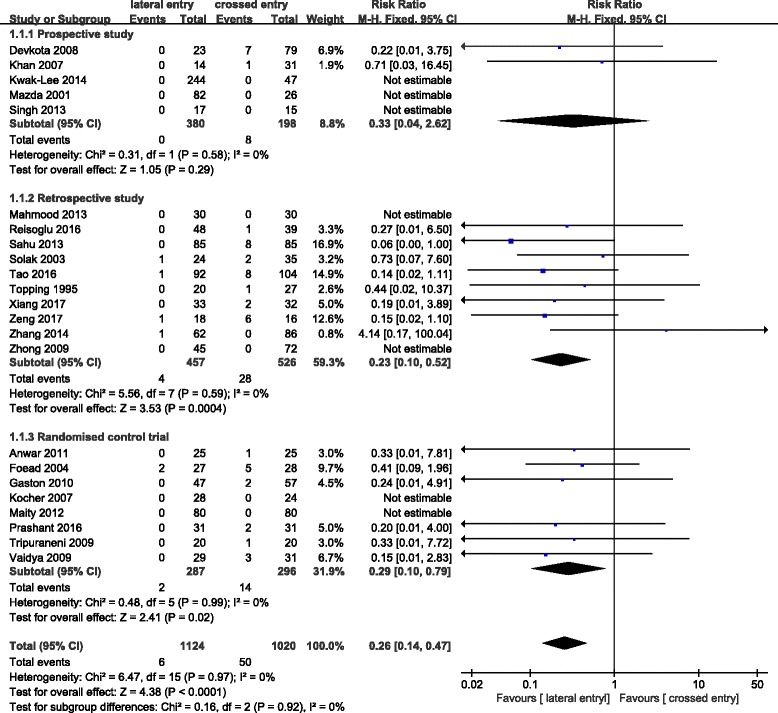
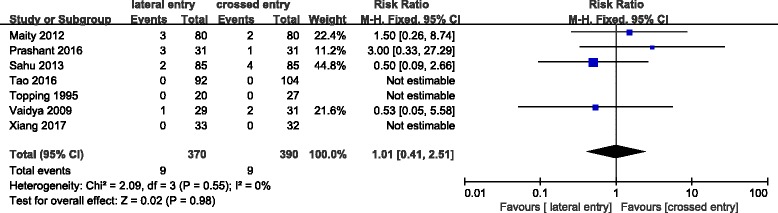
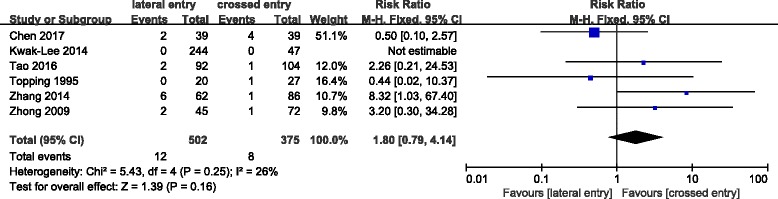
Results: Twenty-four studies were included in the present meta-analysis involving 1163 patients with lateral entry pins and 1059 patients with crossed entry pins. An excellent score of Flynn criteria occurred more commonly in patients who treated with crossed pins than in patients with lateral pins only (RR = 0.93; 95% CI 0.87-0.99; P = 0.03). In accordance with previous systematic review, the incidence of iatrogenic ulnar nerve injury in crossed entry group was significantly more than in lateral entry group with statistical difference (RR = 0.26; 95% CI 0.14-0.47; P < 0.0001). And, results of subgroup analysis on iatrogenic ulnar nerve injury based on experimental design of retrospective study (RR = 0.23; 95% CI 0.10-0.52; P < 0.0004) and randomized control trial (RR = 0.29; 95% CI 0.10-0.79; P < 0.02) were similar.
Conclusions: In consideration of the contradictoriness of lateral entry with two pins only (possible risk of poor functional consequence of elbow) and crossed entry pins (risk of iatrogenic ulnar nerve injury), the recommended strategy for the treatment of SCHF is the lateral entry technique with introducing divergent three pins which can provide a stable configuration and avoid the injury of the ulnar nerve. And additional protective measures for the ulnar nerve should be taken by surgeons that wish for the more stable structure with the crossed entry technique.
Keywords: Pediatric; Pin fixation; Supracondylar humeral fracture.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable. This meta-analysis does not involve research on humans.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet. 1959;109:145–154. - PubMed
-
- Cheng JC, Lam TP, Maffulli N. Epidemiological features of supracondylar fractures of the humerus in Chinese children. J Pediatr Orthop B. 2001;10:63–67. - PubMed
-
- Millis MB, Singer IJ, Hall JE. Supracondylar fracture of the humerus in children. Further experience with a study in orthopaedic decision-making. Clin Orthop Relat Res. 1984;188:90–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
