

Decreased risk adjusted 30-day mortality for hospital admitted injuries: a multi-centre longitudinal study
- PMID: 29615089
- PMCID: PMC5883358
- DOI: 10.1186/s13049-018-0485-2
Decreased risk adjusted 30-day mortality for hospital admitted injuries: a multi-centre longitudinal study
Abstract
Background: The interpretation of changes in injury-related mortality over time requires an understanding of changes in the incidence of the various types of injury, and adjustment for their severity. Our aim was to investigate changes over time in incidence of hospital admission for injuries caused by falls, traffic incidents, or assaults, and to assess the risk-adjusted short-term mortality for these patients.
Methods: All patients admitted to hospital with injuries caused by falls, traffic incidents, or assaults during the years 2001-11 in Sweden were identified from the nationwide population-based Patient Registry. The trend in mortality over time for each cause of injury was adjusted for age, sex, comorbidity and severity of injury as classified from the International Classification of diseases, version 10 Injury Severity Score (ICISS).
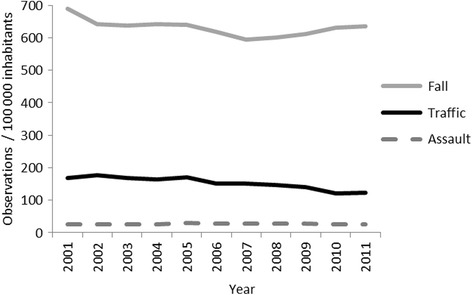
Results: Both the incidence of fall (689 to 636/100000 inhabitants: p = 0.047, coefficient - 4.71) and traffic related injuries (169 to 123/100000 inhabitants: p < 0.0001, coefficient - 5.37) decreased over time while incidence of assault related injuries remained essentially unchanged during the study period. There was an overall decrease in risk-adjusted 30-day mortality in all three groups (OR 1.00; CI95% 0.99-1.00). Decreases in traffic (OR 0.95; 95% CI 0.93 to 0.97) and assault (OR 0.93; 95% CI 0.87 to 0.99) related injuries was significant whereas falls were not during this 11-year period.
Discussion: Risk-adjustment is a good way to use big materials to find epidemiological changes. However after adjusting for age, year, sex and risk we find that a possible factor is left in the pre- and/or in-hospital care.
Conclusions: The decrease in risk-adjusted mortality may suggest changes over time in pre- and/or in-hospital care. A non-significantdecrease in risk-adjusted mortality was registered for falls, which may indicate that low-energy trauma has not benefited for the increased survivability as much as high-energy trauma, ie traffic- and assault related injuries.
Keywords: Epidemiological; ICISS; Injury; Nationwide; Risk-adjusted mortality; Trauma.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Regional Ethics Review Board in Linkoping, Sweden.
Consent for publication
Not applicable.
Competing interests
No conflicts of interest where declared by the authors. However Rolf Gedeborg is also employed by the Medical Products Agency, an agency of the Swedish government. The views expressed in this paper may not reflect the views of the Medical Products Agency.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


Similar articles
-
Female risk-adjusted survival advantage after injuries caused by falls, traffic or assault: a nationwide 11-year study.Scand J Trauma Resusc Emerg Med. 2019 Mar 15;27(1):24. doi: 10.1186/s13049-019-0597-3. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30871611 Free PMC article.
-
Unintentional injuries: A profile of hospitalization and risk factors for in-hospital mortality in Beijing, China.Injury. 2019 Mar;50(3):663-670. doi: 10.1016/j.injury.2019.01.029. Epub 2019 Jan 18. Injury. 2019. PMID: 30709541
-
Prehospital trauma life support training of ambulance caregivers and the outcomes of traffic-injury victims in Sweden.J Am Coll Surg. 2013 Dec;217(6):1010-9.e1-2. doi: 10.1016/j.jamcollsurg.2013.08.002. Epub 2013 Aug 23. J Am Coll Surg. 2013. PMID: 23978531
-
Unarmed violence-related injuries requiring hospitalization in Sweden from 1987 to 1994.J Trauma. 1999 Oct;47(4):733-7. doi: 10.1097/00005373-199910000-00020. J Trauma. 1999. PMID: 10528610
-
The epidemiology of chronic pain.Pain. 2016 Oct;157(10):2158-2159. doi: 10.1097/j.pain.0000000000000676. Pain. 2016. PMID: 27643833 Review. No abstract available.
Cited by
-
Female risk-adjusted survival advantage after injuries caused by falls, traffic or assault: a nationwide 11-year study.Scand J Trauma Resusc Emerg Med. 2019 Mar 15;27(1):24. doi: 10.1186/s13049-019-0597-3. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30871611 Free PMC article.
-
Impact of hospital type on risk-adjusted, traffic-related 30-day mortality: a population-based registry study.Burns Trauma. 2021 Mar 6;9:tkaa051. doi: 10.1093/burnst/tkaa051. eCollection 2021 Jan. Burns Trauma. 2021. PMID: 33732745 Free PMC article.
-
Evaluation of emergency department admissions of mass casualty patients using the revised trauma score, injury severity score, and trauma and injury severity score.Ulus Travma Acil Cerrahi Derg. 2024 Mar;30(3):192-202. doi: 10.14744/tjtes.2024.73531. Ulus Travma Acil Cerrahi Derg. 2024. PMID: 38506389 Free PMC article.
-
The usefulness of a trauma probability of survival model for forensic life-threatening danger assessments.Int J Legal Med. 2021 May;135(3):871-877. doi: 10.1007/s00414-020-02499-3. Epub 2021 Jan 3. Int J Legal Med. 2021. PMID: 33388971 Free PMC article.
References
-
- Osler TM, Cohen M, Rogers FB, Camp L, Rutledge R, Shackford SR. Trauma registry injury coding is superfluous: a comparison of outcome prediction based on trauma registry International Classification of Diseases-Ninth Revision (ICD-9) and hospital information system ICD-9 codes. J Trauma. 1997;43:253–256. doi: 10.1097/00005373-199708000-00008. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
