

Improving outcomes after pediatric cardiac arrest - the ICU-Resuscitation Project: study protocol for a randomized controlled trial
- PMID: 29615134
- PMCID: PMC5883604
- DOI: 10.1186/s13063-018-2590-y
Improving outcomes after pediatric cardiac arrest - the ICU-Resuscitation Project: study protocol for a randomized controlled trial
Abstract
Background: Quality of cardiopulmonary resuscitation (CPR) is associated with survival, but recommended guidelines are often not met, and less than half the children with an in-hospital arrest will survive to discharge. A single-center before-and-after study demonstrated that outcomes may be improved with a novel training program in which all pediatric intensive care unit staff are encouraged to participate in frequent CPR refresher training and regular, structured resuscitation debriefings focused on patient-centric physiology.
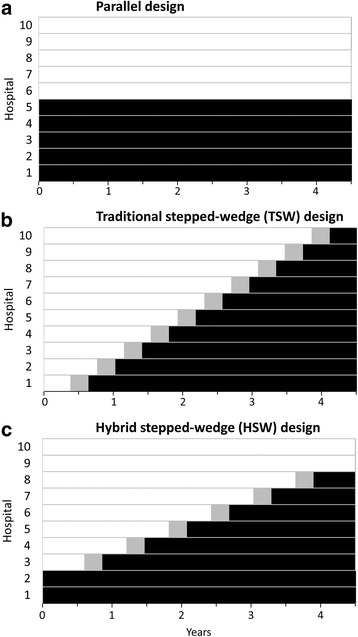
Methods/design: This ongoing trial will assess whether a program of structured debriefings and point-of-care bedside practice that emphasizes physiologic resuscitation targets improves the rate of survival to hospital discharge with favorable neurologic outcome in children receiving CPR in the intensive care unit. This study is designed as a hybrid stepped-wedge trial in which two of ten participating hospitals are randomly assigned to enroll in the intervention group and two are assigned to enroll in the control group for the duration of the trial. The remaining six hospitals enroll initially in the control group but will transition to enrolling in the intervention group at randomly assigned staggered times during the enrollment period.
Discussion: To our knowledge, this is the first implementation of a hybrid stepped-wedge design. It was chosen over a traditional stepped-wedge design because the resulting improvement in statistical power reduces the required enrollment by 9 months (14%). However, this design comes with additional challenges, including logistics of implementing an intervention prior to the start of enrollment. Nevertheless, if results from the single-center pilot are confirmed in this trial, it will have a profound effect on CPR training and quality improvement initiatives.
Trial registration: ClinicalTrials.gov, NCT02837497 . Registered on July 19, 2016.
Keywords: Cardiac arrest; Cardiopulmonary resuscitation (CPR); Hybrid; In-hospital; Pediatric; Stepped-wedge; Survival.
Conflict of interest statement
Ethics approval and consent to participate
This trial was reviewed and approved with waiver of consent by the University of Utah Institutional Review Board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
