

Mortality and detailed characteristics of pre-ICU qSOFA-negative patients with suspected sepsis: an observational study
- PMID: 29616433
- PMCID: PMC5882475
- DOI: 10.1186/s13613-018-0389-3
Mortality and detailed characteristics of pre-ICU qSOFA-negative patients with suspected sepsis: an observational study
Abstract
Background: Recent studies have suggested that quick Sequential Organ Failure Assessment (qSOFA) scores have limited utility in early prognostication in high-mortality populations. The purpose of this study was to investigate the association between pre-ICU qSOFA scores and in-hospital mortality among patients admitted to the ICU with suspected sepsis. This study also aimed to describe detailed clinical characteristics of qSOFA-negative (< 2) patients.
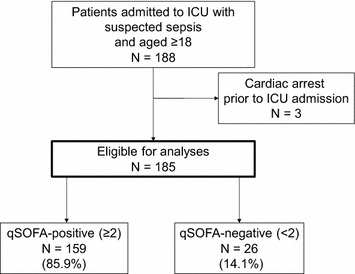
Methods: This single center, observational study, conducted in a Japanese tertiary care teaching hospital between May 2012 and June 2016, enrolled all consecutive adult patients admitted to the ICU with suspected sepsis. We assessed pre-ICU qSOFA scores with the most abnormal vital signs during the 24-h period before ICU admission. The primary outcome was in-hospital mortality censored at 90 days. We analyzed the association between pre-ICU qSOFA scores and in-hospital mortality.
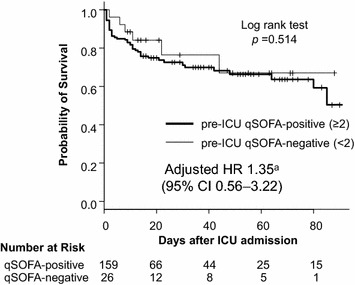
Results: Among 185 ICU patients with suspected sepsis, 14.1% (26/185) of patients remained qSOFA-negative at the time of ICU admission and 29.2% (54/185) of patients died while in hospital. In-hospital mortality was similar between the groups (qSOFA-positive [≥ 2]: 30.2% [48/159] vs qSOFA-negative: 23.1% [6/26], p = 0.642). The Cox proportional hazard regression model revealed that being qSOFA-positive was not significantly associated with in-hospital mortality (adjusted hazard ratio 1.35, 95% confidence interval 0.56-3.22, p = 0.506). Bloodstream infection, immunosuppression, and hematologic malignancy were observed more frequently in qSOFA-negative patients.
Conclusions: Among ICU patients with suspected sepsis, we could not find a strong association between pre-ICU qSOFA scores and in-hospital mortality. Our study suggested high mortality and bacterial diversity in pre-ICU qSOFA-negative patients.
Keywords: Bacteremia; Critical care; Infection; Intensive care unit; Mortality; Sepsis; quick Sequential Organ Failure Assessment (qSOFA) score.
Figures
References
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, Artigas A, Schorr C, Levy MM. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–1755. doi: 10.1097/CCM.0000000000000330. - DOI - PubMed
-
- Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, Rubenfeld G, Kahn JM, Shankar-Hari M, Singer M, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (Sepsis-3) JAMA. 2016;315(8):762–774. doi: 10.1001/jama.2016.0288. - DOI - PMC - PubMed
-
- Churpek MM, Snyder A, Han X, Sokol S, Pettit N, Howell MD, Edelson DP. Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside the intensive care unit. Am J Respir Crit Care Med. 2017;195(7):906–911. doi: 10.1164/rccm.201604-0854OC. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
