

How to use the Kaiser score as a clinical decision rule for diagnosis in multiparametric breast MRI: a pictorial essay
- PMID: 29616496
- PMCID: PMC5990997
- DOI: 10.1007/s13244-018-0611-8
How to use the Kaiser score as a clinical decision rule for diagnosis in multiparametric breast MRI: a pictorial essay
Abstract
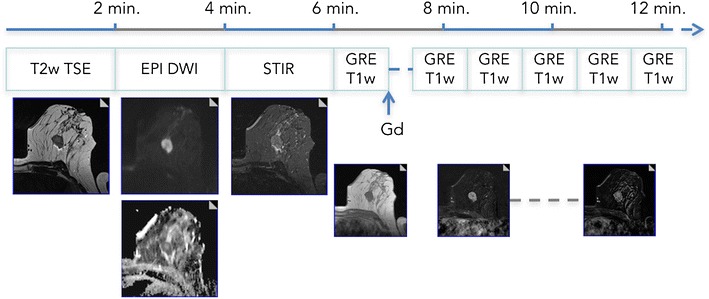
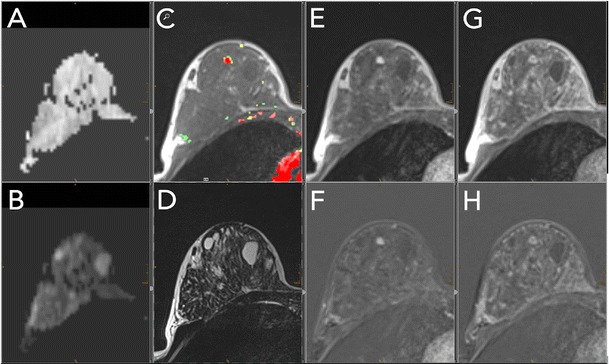
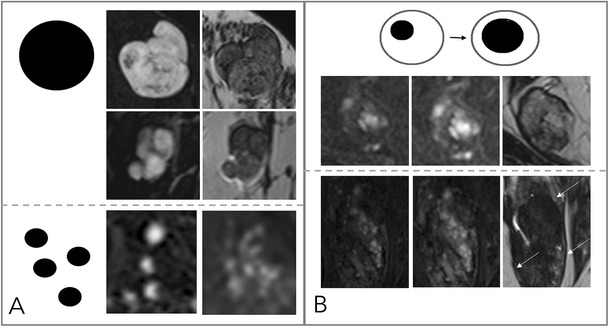
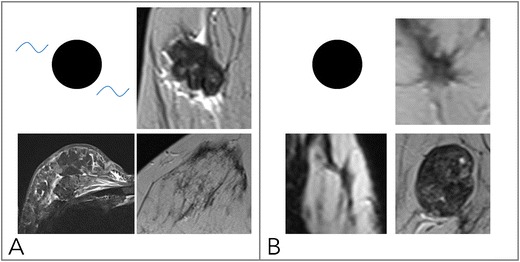
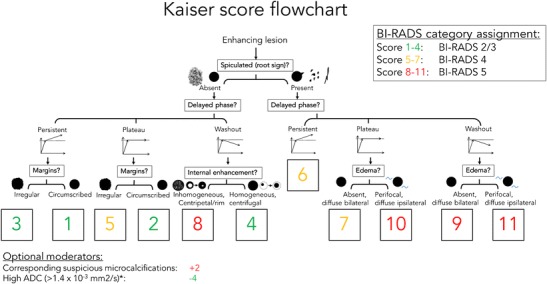
Due to its superior sensitivity, breast MRI (bMRI) has been established as an important additional diagnostic tool in the breast clinic and is used for screening in patients with an elevated risk for breast cancer. Breast MRI, however, is a complex tool, providing multiple images containing several contrasts. Thus, reading bMRI requires a structured approach. A lack of structure will increase the rate of false-positive findings and sacrifice most of the advantages of bMRI as additional work-up will be required. While the BI-RADS (Breast Imaging Reporting And Data System) lexicon is a major step toward standardised and structured reporting, it does not provide a clinical decision rule with which to guide diagnostic decisions. Such a clinical decision rule, however, is provided by the Kaiser score, which combines five independent diagnostic BI-RADS lexicon criteria (margins, SI-time curve type, internal enhancement and presence of oedema) in an intuitive flowchart. The resulting score provides probabilities of malignancy that can be used for evidence-based decision-making in the breast clinic. Notably, considerable benefits have been demonstrated for radiologists with initial and intermediate experience in bMRI. This pictorial essay is a practical guide to the application of the Kaiser score in the interpretation of breast MRI examinations.
Teaching points: • bMRI requires standardisation of patient-management, protocols, and reading set-up. • Reading bMRI includes the assessment of breast parenchyma, associated findings, and lesions. • Diagnostic decisions should be made according to evidence-based clinical decision rules. • The evidence-based Kaiser score is applicable independent of bMRI protocol and scanner. • The Kaiser score provides high diagnostic accuracy with low inter-observer variability.
Keywords: Breast MRI; Breast cancer; Clinical decision-making; Patient management.
Figures




References
-
- Heywang SH, Hilbertz T, Pruss E, et al. Dynamic contrast medium studies with flash sequences in nuclear magnetic resonance tomography of the breast. Digitale Bilddiagn. 1988;8:7–13. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
