

PPAR-gamma activation is associated with reduced liver ischemia-reperfusion injury and altered tissue-resident macrophages polarization in a mouse model
- PMID: 29617419
- PMCID: PMC5884549
- DOI: 10.1371/journal.pone.0195212
PPAR-gamma activation is associated with reduced liver ischemia-reperfusion injury and altered tissue-resident macrophages polarization in a mouse model
Abstract
Background: PPAR-gamma (γ) is highly expressed in macrophages and its activation affects their polarization. The effect of PPAR-γ activation on Kupffer cells (KCs) and liver ischemia-reperfusion injury (IRI) has not yet been evaluated. We investigated the effect of PPAR-γ activation on KC-polarization and IRI.
Materials and methods: Seventy percent (70%) liver ischemia was induced for 60mins. PPAR-γ-agonist or vehicle was administrated before reperfusion. PPAR-γ-antagonist was used to block PPAR-γ activation. Liver injury, necrosis, and apoptosis were assessed post-reperfusion. Flow-cytometry determined KC-phenotypes (pro-inflammatory Nitric Oxide +, anti-inflammatory CD206+ and anti-inflammatory IL-10+).
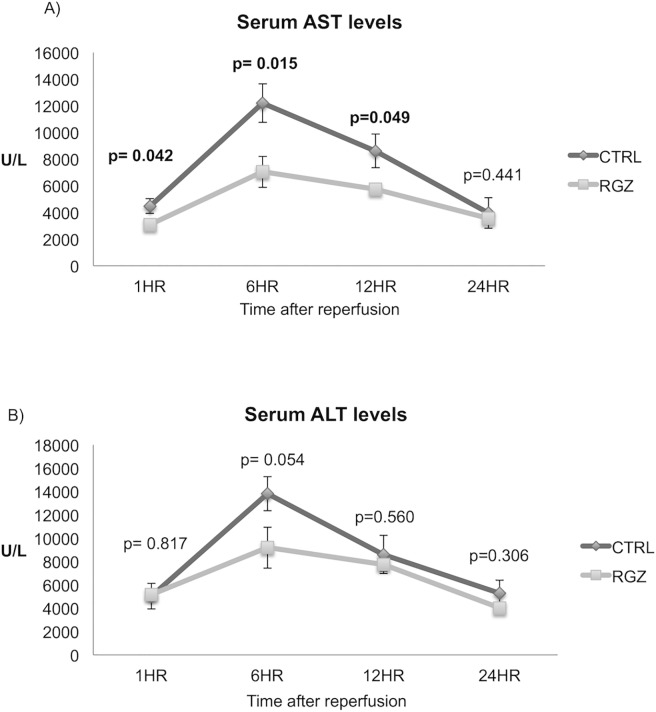
Results: Liver injury assessed by serum AST was significantly decreased in PPAR-γ-agonist versus control group at all time points post reperfusion (1hr: 3092±105 vs 4469±551; p = 0.042; 6hr: 7041±1160 vs 12193±1143; p = 0.015; 12hr: 5746±328 vs 8608±1259; p = 0.049). Furthermore, liver apoptosis measured by TUNEL-staining was significantly reduced in PPAR-γ-agonist versus control group post reperfusion (1hr:2.46±0.49 vs 6.90±0.85%;p = 0.001; 6hr:26.40±2.93 vs 50.13±8.29%; p = 0.048). H&E staining demonstrated less necrosis in PPAR-γ-agonist versus control group (24hr:26.66±4.78 vs 45.62±4.57%; p = 0.032). The percentage of pro-inflammatory NO+ KCs was significantly lower at all post reperfusion time points in the PPAR-γ-agonist versus control group (1hr:28.49±4.99 vs 53.54±9.15%; p = 0.040; 6hr:5.51±0.54 vs 31.12±9.58%; p = 0.009; 24hr:4.15±1.50 vs 17.10±4.77%; p = 0.043). In contrast, percentage of anti-inflammatory CD206+ KCs was significantly higher in PPAR-γ-agonist versus control group prior to IRI (8.62±0.96 vs 4.88 ±0.50%; p = 0.04). Administration of PPAR-γ-antagonist reversed the beneficial effects on AST, apoptosis, and pro-inflammatory NO+ KCs.
Conclusion: PPAR-γ activation reduces IRI and decreases the pro-inflammatory NO+ Kupffer cells. PPAR-γ activation can become an important tool to improve outcomes in liver surgery through decreasing the pro-inflammatory phenotype of KCs and IRI.
Conflict of interest statement
Figures








Similar articles
-
15-hydroxyprostaglandin dehydrogenase (15-PGDH) prevents lipopolysaccharide (LPS)-induced acute liver injury.PLoS One. 2017 Apr 19;12(4):e0176106. doi: 10.1371/journal.pone.0176106. eCollection 2017. PLoS One. 2017. PMID: 28423012 Free PMC article.
-
MicroRNA-155 Deficiency in Kupffer Cells Ameliorates Liver Ischemia-Reperfusion Injury in Mice.Transplantation. 2017 Jul;101(7):1600-1608. doi: 10.1097/TP.0000000000001765. Transplantation. 2017. PMID: 28640790
-
Activation of PPARγ by Curcumin protects mice from ischemia/reperfusion injury induced by orthotopic liver transplantation via modulating polarization of Kupffer cells.Int Immunopharmacol. 2018 Sep;62:270-276. doi: 10.1016/j.intimp.2018.07.013. Epub 2018 Jul 23. Int Immunopharmacol. 2018. PMID: 30036770
-
Novel Targets for Treating Ischemia-Reperfusion Injury in the Liver.Int J Mol Sci. 2018 Apr 26;19(5):1302. doi: 10.3390/ijms19051302. Int J Mol Sci. 2018. PMID: 29701719 Free PMC article. Review.
-
Effect of Hepatic Macrophage Polarization and Apoptosis on Liver Ischemia and Reperfusion Injury During Liver Transplantation.Front Immunol. 2020 Jun 26;11:1193. doi: 10.3389/fimmu.2020.01193. eCollection 2020. Front Immunol. 2020. PMID: 32676077 Free PMC article. Review.
Cited by
-
PPARγ in Ischemia-Reperfusion Injury: Overview of the Biology and Therapy.Front Pharmacol. 2021 Apr 28;12:600618. doi: 10.3389/fphar.2021.600618. eCollection 2021. Front Pharmacol. 2021. PMID: 33995008 Free PMC article. Review.
-
Dual Effect of Hepatic Macrophages on Liver Ischemia and Reperfusion Injury during Liver Transplantation.Immune Netw. 2018 Jun 28;18(3):e24. doi: 10.4110/in.2018.18.e24. eCollection 2018 Jun. Immune Netw. 2018. PMID: 29984042 Free PMC article. Review.
-
PPAR Gamma: From Definition to Molecular Targets and Therapy of Lung Diseases.Int J Mol Sci. 2021 Jan 15;22(2):805. doi: 10.3390/ijms22020805. Int J Mol Sci. 2021. PMID: 33467433 Free PMC article. Review.
-
An Overview of the Role of Peroxisome Proliferator-activated Receptors in Liver Diseases.J Clin Transl Hepatol. 2023 Dec 28;11(7):1542-1552. doi: 10.14218/JCTH.2023.00334. Epub 2023 Nov 15. J Clin Transl Hepatol. 2023. PMID: 38161499 Free PMC article. Review.
-
Rosiglitazone Protects against Acetaminophen-Induced Acute Liver Injury by Inhibiting Multiple Endoplasmic Reticulum Stress Pathways.Biomed Res Int. 2022 Dec 21;2022:6098592. doi: 10.1155/2022/6098592. eCollection 2022. Biomed Res Int. 2022. PMID: 36588533 Free PMC article.
References
-
- Jaeschke H. Molecular mechanisms of hepatic ischemia-reperfusion injury and preconditioning. Am J Physiol Gastrointest Liver Physiol. 2003;284(1):G15–26. doi: 10.1152/ajpgi.00342.2002 . - DOI - PubMed
-
- Fondevila C, Busuttil RW, Kupiec-Weglinski JW. Hepatic ischemia/reperfusion injury—a fresh look. Exp Mol Pathol. 2003;74(2):86–93. . - PubMed
-
- Clavien PA, Rudiger HA, Selzner M. Mechanism of hepatocyte death after ischemia: apoptosis versus necrosis. Hepatology. 2001;33(6):1555–7. doi: 10.1053/jhep.2001.0103306le02 . - DOI - PubMed
-
- Selzner N, Rudiger H, Graf R, Clavien PA. Protective strategies against ischemic injury of the liver. Gastroenterology. 2003;125(3):917–36. . - PubMed
-
- Bendinelli P, Piccoletti R, Maroni P, Bernelli-Zazzera A. The MAP kinase cascades are activated during post-ischemic liver reperfusion. FEBS Lett. 1996;398(2–3):193–7. . - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
