

Clinical and Laboratory Predictors of Shiga Toxin-Producing Escherichia coli Infection in Children With Bloody Diarrhea
- PMID: 29617871
- PMCID: PMC6097574
- DOI: 10.1093/jpids/piy025
Clinical and Laboratory Predictors of Shiga Toxin-Producing Escherichia coli Infection in Children With Bloody Diarrhea
Abstract
Objectives: Children with acute bloody diarrhea are at risk of being infected with Shiga toxin-producing Escherichia coli (STEC) and of progression to hemolytic uremic syndrome. Our objective was to identify clinical and laboratory factors associated with STEC infection in children who present with acute bloody diarrhea.
Methods: We performed a prospective cohort study of consecutive children younger than 18 years who presented with acute (<2-week duration) bloody diarrhea between August 1, 2013, and August 1, 2014. We excluded patients with a chronic gastrointestinal illness and/or an obvious noninfectious source of bloody stool. We obtained a standardized history and study laboratory tests, performed physical examinations, and recorded patient outcomes.
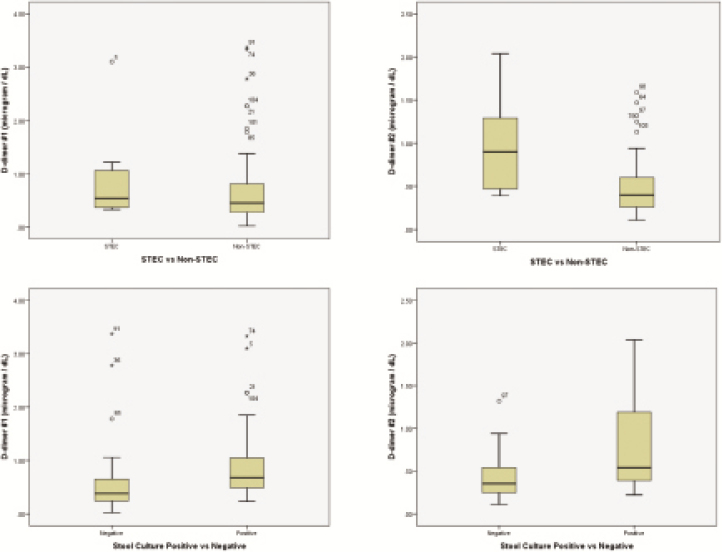
Results: Of the 135 eligible patients, 108 were enrolled; 27 declined consent. The median patient age was 3 years, and 56% were male. Ten (9%) patients tested positive for STEC (E coli O157:H7, n = 8; E coli O111, n = 1; E coli O103, n = 1), and 62 had negative stool culture results. Children infected with STEC were older (8.5 vs 3 years, respectively) (P < .001) and more likely to have abdominal tenderness (83% vs 17%, respectively) than those in the other groups. D-Dimer concentrations had a 70% sensitivity and 55% specificity for differentiating children with STEC from those with another cause of bloody diarrhea and 75% sensitivity and 70% specificity in differentiating children with a bacterial etiology from those with negative stool culture results.
Conclusion: Clinical assessment and laboratory data cannot reliably exclude the possibility that children with bloody diarrhea have an STEC infection and are at consequent risk of developing hemolytic uremic syndrome. Abnormal D-dimer concentrations (>0.5 μg/mL) were insufficiently sensitive and specific for distinguishing patients with STEC from those with another bacterial cause of bloody diarrhea. However, this marker might be useful in identifying children whose bloody diarrhea is caused by a bacterial enteric pathogen.
Figures
References
-
- Holtz LR, Neill MA, Tarr PI. Acute bloody diarrhea: a medical emergency for patients of all ages. Gastroenterology 2009; 136:1887–98. - PubMed
-
- Klein EJ, Stapp JR, Clausen CR, et al. Shiga toxin–producing Escherichia coli in children with diarrhea: a prospective point-of-care study. J Pediatr 2002; 141:172–7. - PubMed
-
- Chandler WL, Jelacic S, Boster DR, et al. Prothrombotic coagulation abnormalities preceding the hemolytic-uremic syndrome. N Engl J Med 2002; 346:23–32. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
