

The role of FREM2 and FRAS1 in the development of congenital diaphragmatic hernia
- PMID: 29618029
- PMCID: PMC5985720
- DOI: 10.1093/hmg/ddy110
The role of FREM2 and FRAS1 in the development of congenital diaphragmatic hernia
Abstract
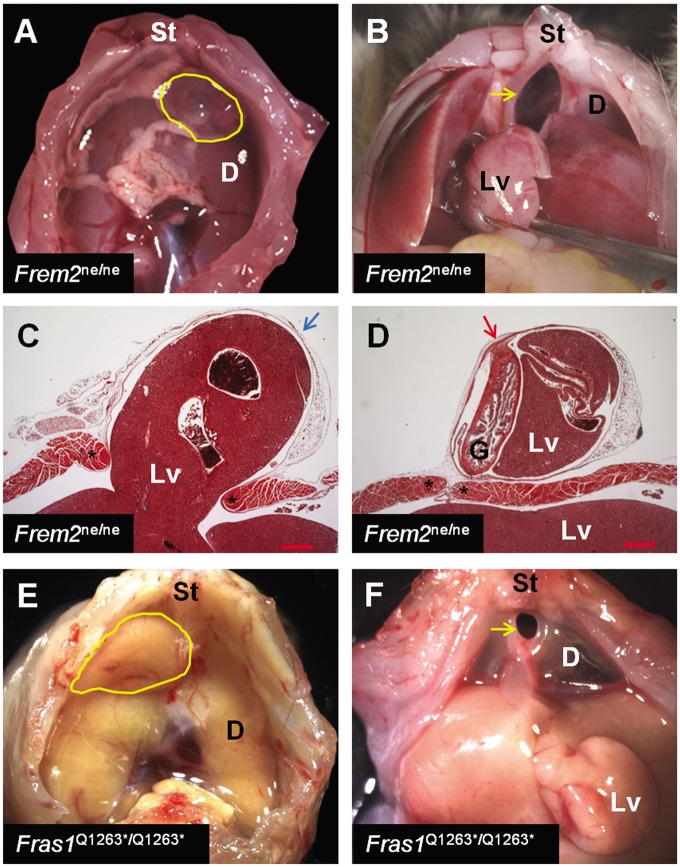
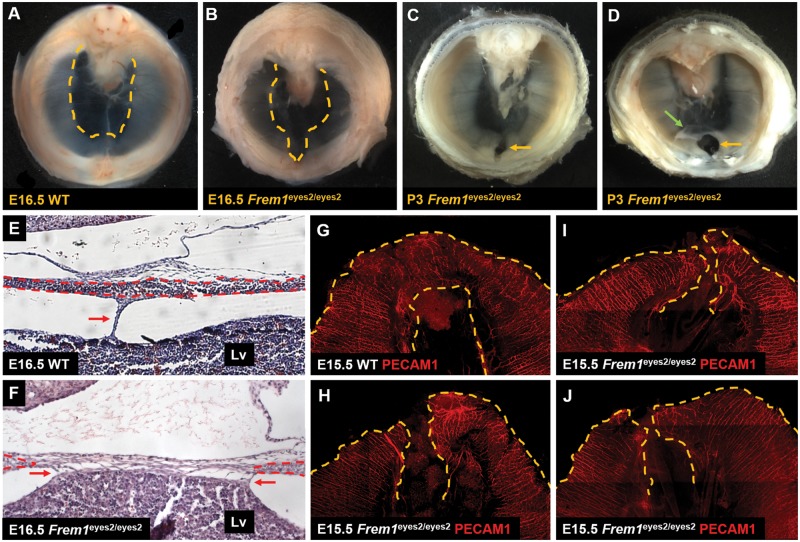
Congenital diaphragmatic hernia (CDH) has been reported twice in individuals with a clinical diagnosis of Fraser syndrome, a genetic disorder that can be caused by recessive mutations affecting FREM2 and FRAS1. In the extracellular matrix, FREM2 and FRAS1 form a self-stabilizing complex with FREM1, a protein whose deficiency causes sac CDH in humans and mice. By sequencing FREM2 and FRAS1 in a CDH cohort, and searching online databases, we identified five individuals who carried recessive or double heterozygous, putatively deleterious variants in these genes which may represent susceptibility alleles. Three of these alleles were significantly enriched in our CDH cohort compared with ethnically matched controls. We subsequently demonstrated that 8% of Frem2ne/ne and 1% of Fras1Q1263*/Q1263* mice develop the same type of anterior sac CDH seen in FREM1-deficient mice. We went on to show that development of sac hernias in FREM1-deficient mice is preceded by failure of anterior mesothelial fold progression resulting in the persistence of an amuscular, poorly vascularized anterior diaphragm that is abnormally adherent to the underlying liver. Herniation occurs in the perinatal period when the expanding liver protrudes through this amuscular region of the anterior diaphragm that is juxtaposed to areas of muscular diaphragm. Based on these data, we conclude that deficiency of FREM2, and possibly FRAS1, are associated with an increased risk of developing CDH and that loss of the FREM1/FREM2/FRAS1 complex, or its function, leads to anterior sac CDH development through its effects on mesothelial fold progression.
Figures
References
-
- Skari H., Bjornland K., Haugen G., Egeland T., Emblem R. (2000) Congenital diaphragmatic hernia: a meta-analysis of mortality factors. J. Pediatr. Surg., 35, 1187–1197. - PubMed
-
- Langham M.R. Jr, Kays D.W., Ledbetter D.J., Frentzen B., Sanford L.L., Richards D.S. (1996) Congenital diaphragmatic hernia. Epidemiology and outcome. Clin. Perinatol., 23, 671–688. - PubMed
-
- Zamora I.J., Cass D.L., Lee T.C., Welty S., Cassady C.I., Mehollin-Ray A.R., Fallon S.C., Ruano R., Belfort M.A., Olutoye O.O. (2013) The presence of a hernia sac in congenital diaphragmatic hernia is associated with better fetal lung growth and outcomes. J. Pediatr. Surg., 48, 1165–1171. - PubMed
-
- Bollmann R., Kalache K., Mau H., Chaoui R., Tennstedt C. (1995) Associated malformations and chromosomal defects in congenital diaphragmatic hernia. Fetal Diagn. Ther., 10, 52–59. - PubMed
-
- Tibboel D., Gaag A.V. (1996) Etiologic and genetic factors in congenital diaphragmatic hernia. Clin. Perinatol., 23, 689–699. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
