

Percutaneous vertebroplasty for osteoporotic vertebral compression fracture
- PMID: 29618171
- PMCID: PMC6494647
- DOI: 10.1002/14651858.CD006349.pub3
Percutaneous vertebroplasty for osteoporotic vertebral compression fracture
Update in
-
Percutaneous vertebroplasty for osteoporotic vertebral compression fracture.Cochrane Database Syst Rev. 2018 Nov 6;11(11):CD006349. doi: 10.1002/14651858.CD006349.pub4. Cochrane Database Syst Rev. 2018. PMID: 30399208 Free PMC article.
Abstract
Background: Percutaneous vertebroplasty remains widely used to treat osteoporotic vertebral fractures although our 2015 Cochrane review did not support its role in routine practice.
Objectives: To update the available evidence of the benefits and harms of vertebroplasty for treatment of osteoporotic vertebral fractures.
Search methods: We updated the search of CENTRAL, MEDLINE and Embase and trial registries to 15 November 2017.
Selection criteria: We included randomised and quasi-randomised controlled trials (RCTs) of adults with painful osteoporotic vertebral fractures, comparing vertebroplasty with placebo (sham), usual care, or another intervention. As it is least prone to bias, vertebroplasty compared with placebo was the primary comparison. Major outcomes were mean overall pain, disability, disease-specific and overall health-related quality of life, patient-reported treatment success, new symptomatic vertebral fractures and number of other serious adverse events.
Data collection and analysis: We used standard methodologic procedures expected by Cochrane.
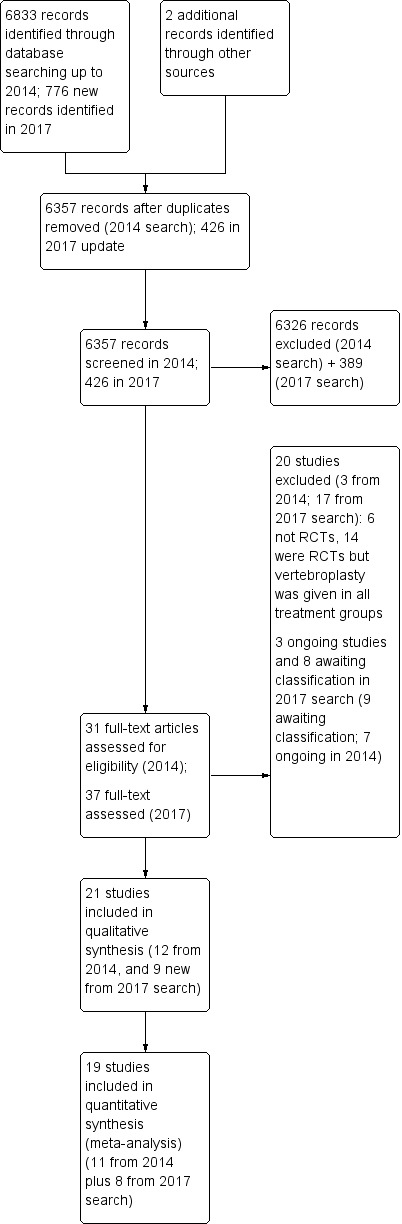
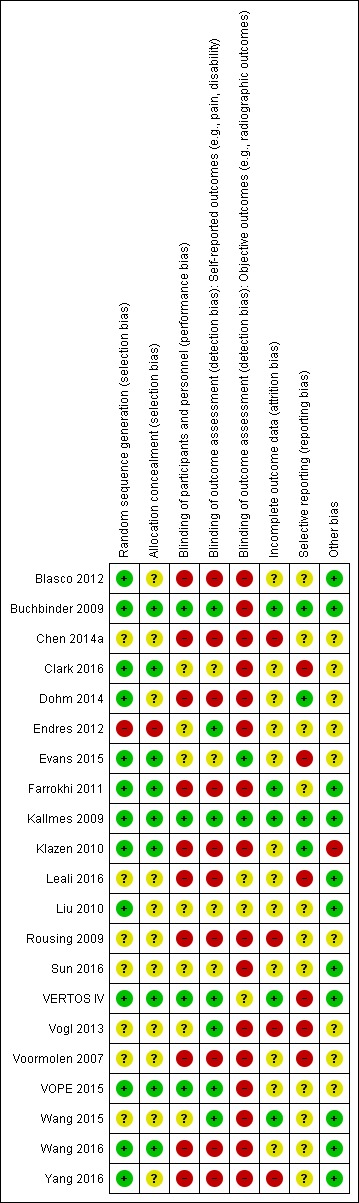
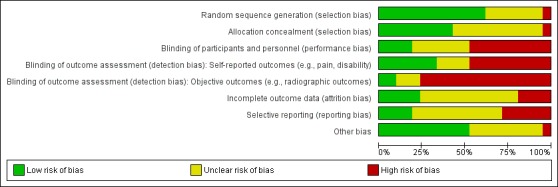
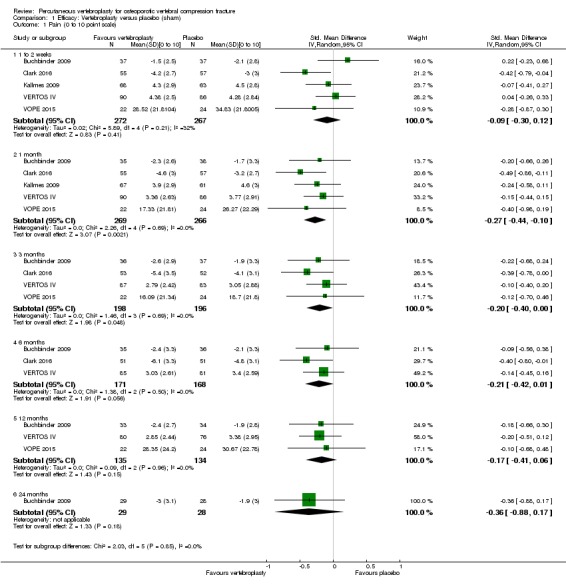
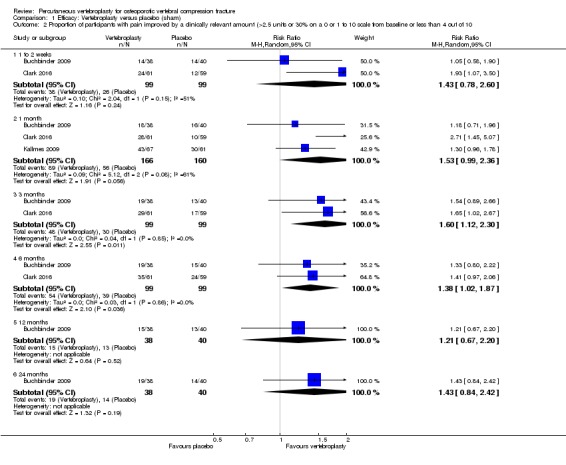
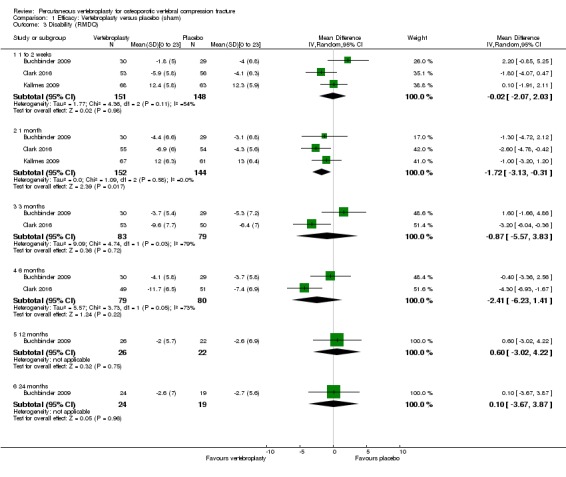
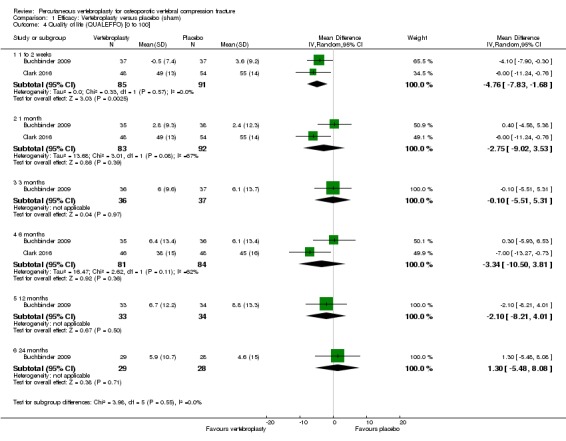
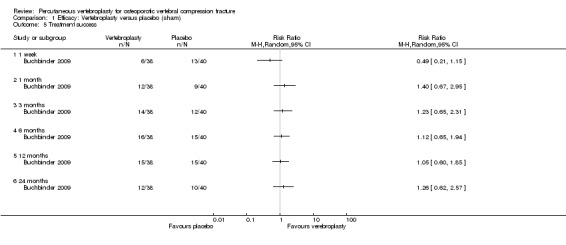
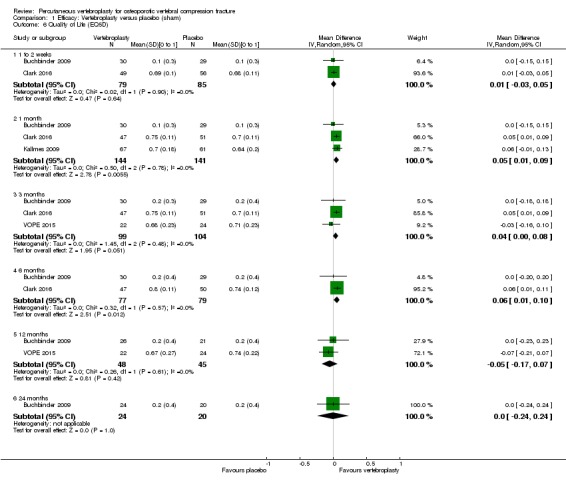
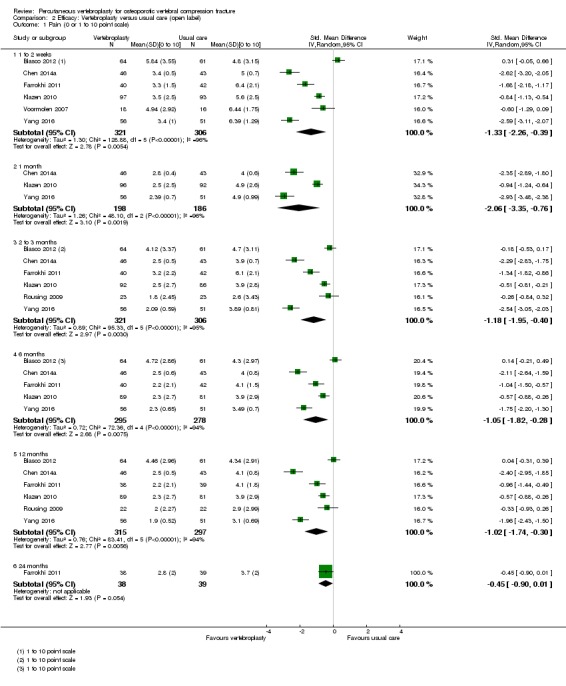
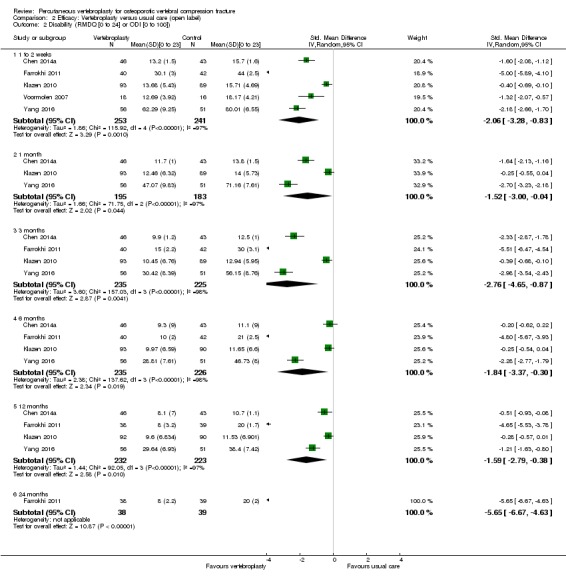
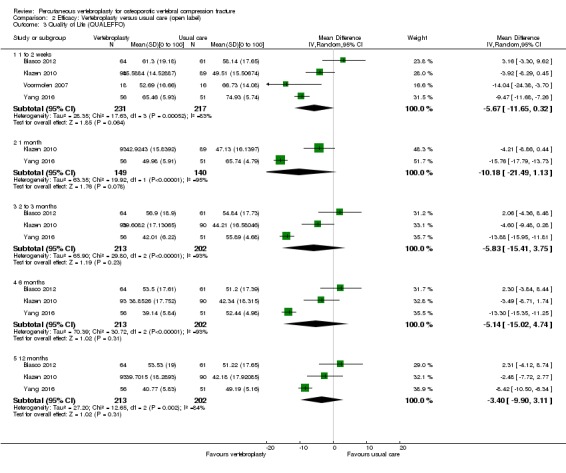
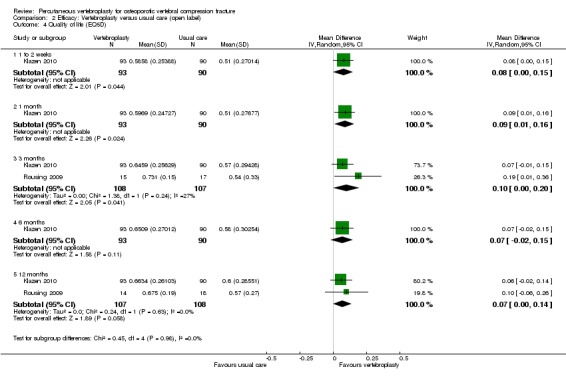
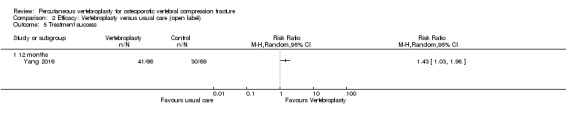
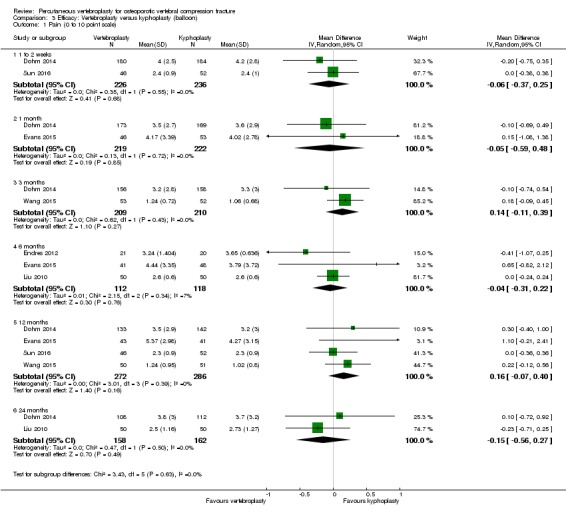
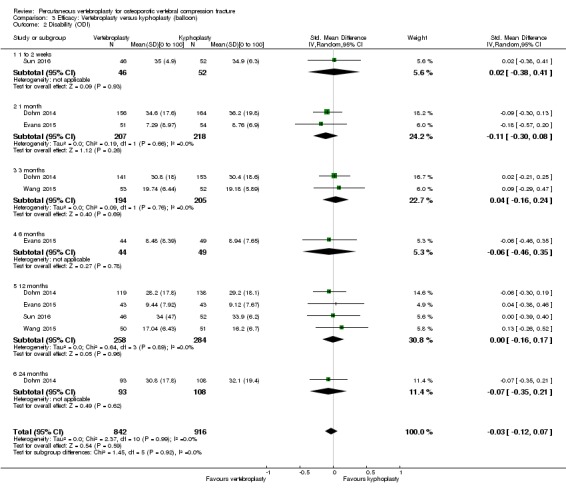
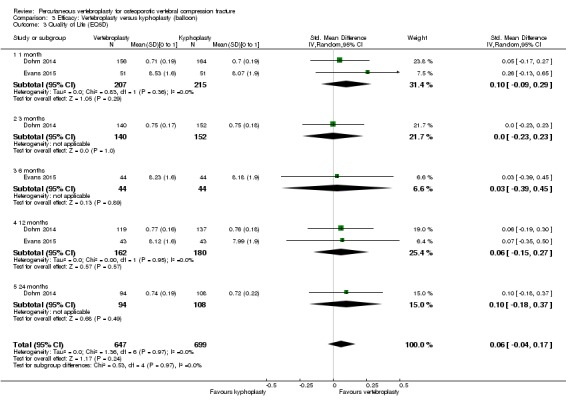
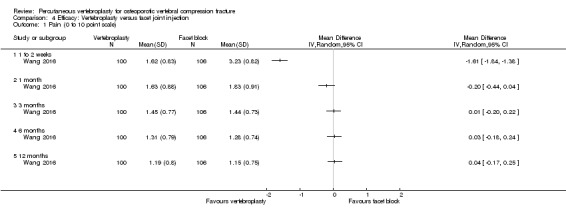
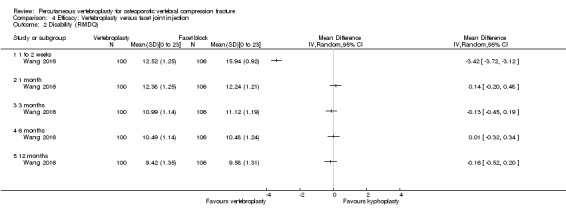
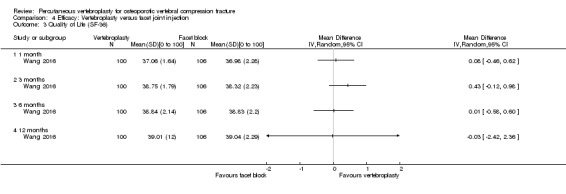
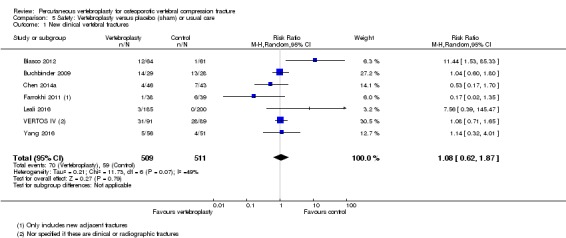
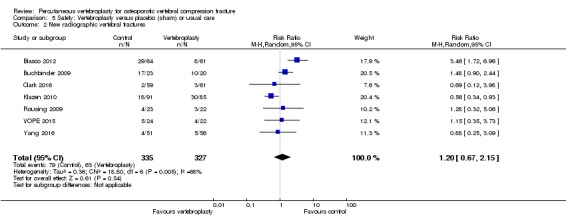
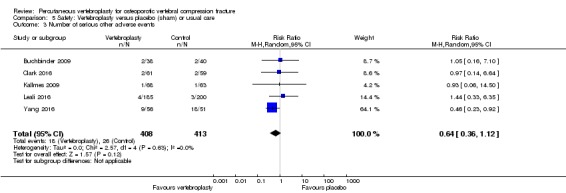
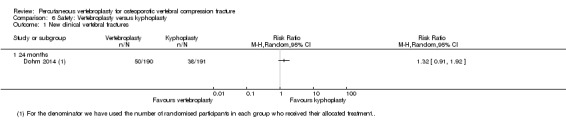
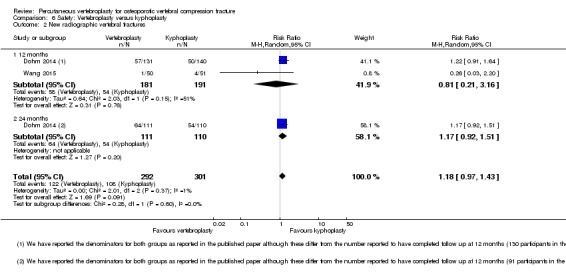
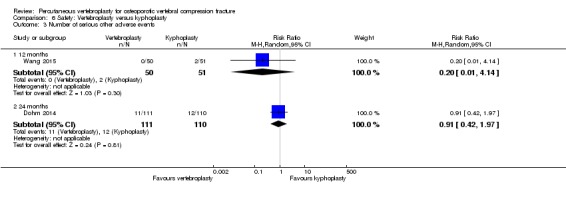
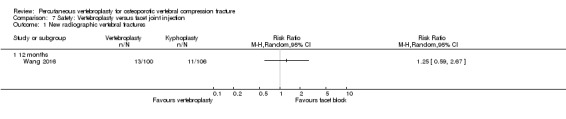
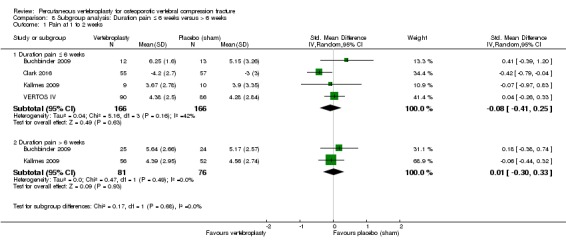
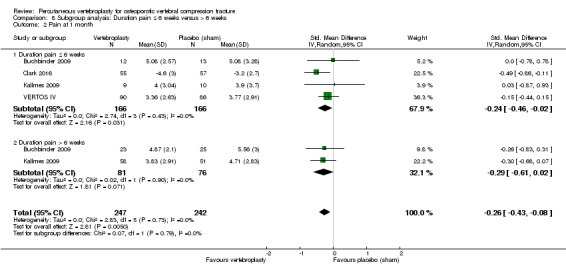
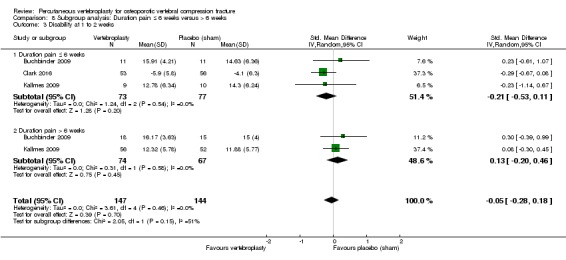
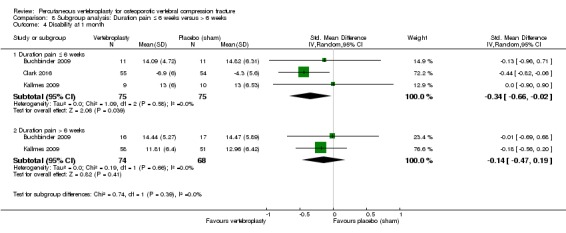
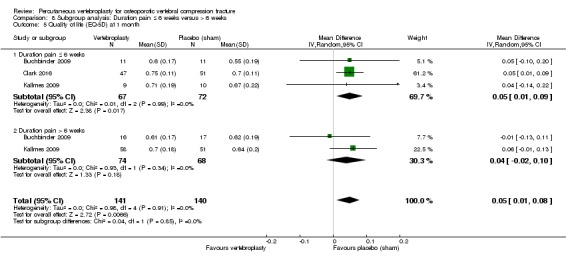
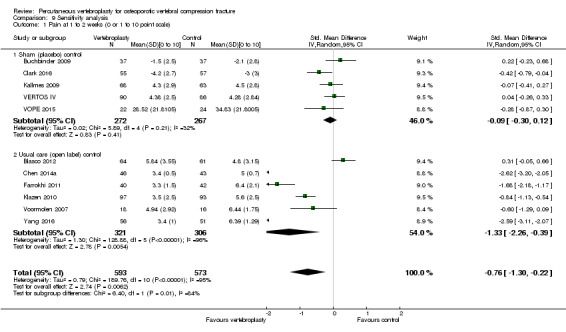
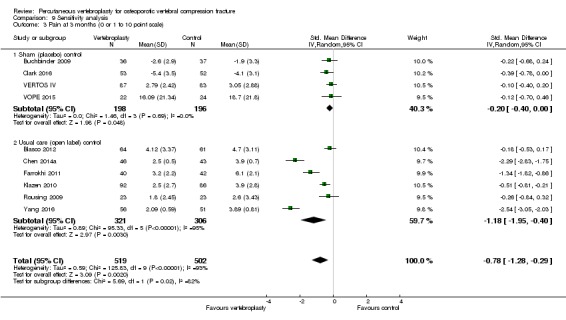
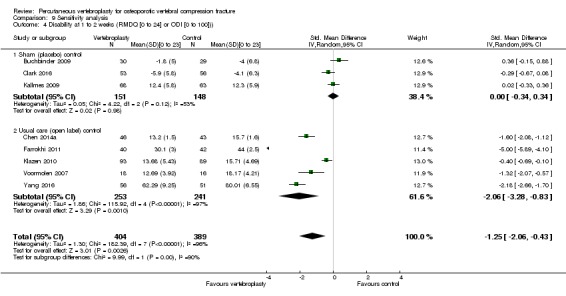
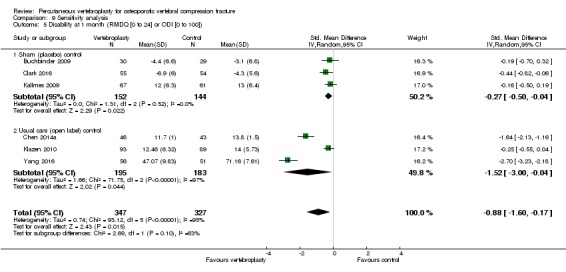
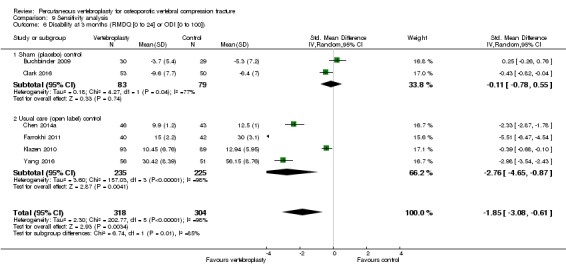
Main results: Twenty-one trials were included: five compared vertebroplasty with placebo (541 randomised participants), eight with usual care (1136 randomised participants), seven with kyphoplasty (968 randomised participants) and one compared vertebroplasty with facet joint glucocorticoid injection (217 randomised participants). Trial size varied from 46 to 404 participants, most participants were female, mean age ranged between 62.6 and 81 years, and mean symptom duration varied from a week to more than six months.Three placebo-controlled trials were at low risk of bias and two were possibly susceptible to performance and detection bias. Other trials were at risk of bias for several criteria, most notably due to lack of participant and personnel blinding.Compared with placebo, high- to moderate-quality evidence from five trials (one with incomplete data reported) indicates that vertebroplasty provides no clinically important benefits with respect to pain, disability, disease-specific or overall quality of life or treatment success at one month. Evidence for quality of life and treatment success was downgraded due to possible imprecision. Evidence was not downgraded for potential publication bias as only one placebo-controlled trial remains unreported. Mean pain (on a scale zero to 10, higher scores indicate more pain) was five points with placebo and 0.6 points better (0.2 better to 1 better) with vertebroplasty, an absolute pain reduction of 6% (2% better to 10% better, minimal clinical important difference is 15%) and relative reduction of 9% (3% better to14% better) (five trials, 535 participants). Mean disability measured by the Roland-Morris Disability Questionnaire (scale range zero to 23, higher scores indicate worse disability) was 14.2 points in the placebo group and 1.7 points better (0.3 better to 3.1 better) in the vertebroplasty group, absolute improvement 7% (1% to 14% better), relative improvement 10% better (3% to 18% better) (three trials, 296 participants).Disease-specific quality of life measured by the Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO) (scale zero to 100, higher scores indicating worse quality of life) was 62 points in the placebo group and 2.75 points (3.53 worse to 9.02 better) in the vertebroplasty group, absolute change: 3% better (4% worse to 9% better), relative change: 5% better (6% worse to 15% better (two trials, 175 participants). Overall quality of life (European Quality of Life (EQ5D), zero = death to 1 = perfect health, higher scores indicate greater quality of life) was 0.38 points in the placebo group and 0.05 points better (0.01 better to 0.09 better) in the vertebroplasty group, absolute improvement: 5% (1% to 9% better), relative improvement: 18% (4% to 32% better) (three trials, 285 participants). In one trial (78 participants), 9/40 (or 225 per 1000) people perceived that treatment was successful in the placebo group compared with 12/38 (or 315 per 1000; 95% CI 150 to 664) in the vertebroplasty group, RR 1.40 (95% CI 0.67 to 2.95), absolute difference: 9% more reported success (11% fewer to 29% more); relative change: 40% more reported success (33% fewer to 195% more).Moderate-quality evidence (low number of events) from seven trials (four placebo, three usual care, 1020 participants), up to 24 months follow-up, indicates we are uncertain whether vertebroplasty increases the risk of new symptomatic vertebral fractures (70/509 (or 130 per 1000; range 60 to 247) observed in the vertebroplasty group compared with 59/511 (120 per 1000) in the control group; RR 1.08 (95% CI 0.62 to 1.87)).Similarly, moderate-quality evidence (low number of events) from five trials (three placebo, two usual care, 821 participants), indicates uncertainty around the risk of other serious adverse events (18/408 or 76 per 1000, range 6 to 156) in the vertebroplasty group compared with 26/413 (or 106 per 1000) in the control group; RR 0.64 (95% CI 0.36 to 1.12). Notably, serious adverse events reported with vertebroplasty included osteomyelitis, cord compression, thecal sac injury and respiratory failure.Our subgroup analyses indicate that the effects did not differ according to duration of pain ≤ 6 weeks versus > 6 weeks. Including data from the eight trials that compared vertebroplasty with usual care in a sensitivity analyses altered the primary results, with all combined analyses displaying considerable heterogeneity.
Authors' conclusions: Based upon high- to moderate-quality evidence, our updated review does not support a role for vertebroplasty for treating acute or subacute osteoporotic vertebral fractures in routine practice. We found no demonstrable clinically important benefits compared with placebo (sham procedure) and subgroup analyses indicated that the results did not differ according to duration of pain ≤ 6 weeks versus > 6 weeks.Sensitivity analyses confirmed that open trials comparing vertebroplasty with usual care are likely to have overestimated any benefit of vertebroplasty. Correcting for these biases would likely drive any benefits observed with vertebroplasty towards the null, in keeping with findings from the placebo-controlled trials.Numerous serious adverse events have been observed following vertebroplasty. However due to the small number of events, we cannot be certain about whether or not vertebroplasty results in a clinically important increased risk of new symptomatic vertebral fractures and/or other serious adverse events. Patients should be informed about both the high- to moderate-quality evidence that shows no important benefit of vertebroplasty and its potential for harm.
Conflict of interest statement
R Buchbinder was a principal investigator of Buchbinder 2009. D Kallmes was a principal investigator of Kallmes 2009 and
Figures

Update of
-
Percutaneous vertebroplasty for osteoporotic vertebral compression fracture.Cochrane Database Syst Rev. 2015 Apr 30;(4):CD006349. doi: 10.1002/14651858.CD006349.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2018 Apr 04;4:CD006349. doi: 10.1002/14651858.CD006349.pub3. PMID: 25923524 Updated.
Comment in
-
Cochrane in CORR®: Percutaneous Vertebroplasty for Osteoporotic Vertebral Compression Fracture.Clin Orthop Relat Res. 2018 Oct;476(10):1920-1927. doi: 10.1097/CORR.0000000000000430. Clin Orthop Relat Res. 2018. PMID: 30211707 Free PMC article. No abstract available.
References
References to studies included in this review
-
- Blasco J, Martinez‐Ferrer A, Macho J, San Roman L, Pomes J, Carrasco J, et al. Effect of vertebroplasty on pain relief, quality of life, and the incidence of new vertebral fractures: a 12‐month randomized follow‐up, controlled trial. Journal of Bone and Mineral Research 2012;27(5):1159‐66. - PubMed
- Blasco J, Martinez‐Ferrer A, San Roman J, Macho A, Lopez Rueda D, Campodonico C, et al. Risk factors for the development of chronic back pain after percutaneous vertebroplasty. European Society of Radiology. 2014.
- Peris P, Blasco J, Carrasco JL, Martinez‐Ferrer A, Macho J, San Roman L, et al. Risk factors for the development of chronic back pain after percutaneous vertebroplasty versus conservative treatment. Calcified Tissue International 2015;96(2):89‐96. - PubMed
-
- Buchbinder R, Osborne RH, Ebeling PR, Wark JD, Mitchell P, Wriedt C, et al. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures.[see comment]. New England Journal of Medicine 2009;361(6):557‐68. - PubMed
- Buchbinder R, Osborne RH, Ebeling PR, Wark JD, Mitchell P, Wriedt CJ, et al. Efficacy and safety of vertebroplasty for treatment of painful osteoporotic vertebral fractures: a randomised controlled trial [ACTRN012605000079640]. BMC Musculoskeletal Disorders 2008;9:156. - PMC - PubMed
- Kroon F, Staples MP, Ebeling P, Wark J, Osborne R, Mitchell P, et al. Vertebroplasty for osteoporotic vertebral fractures: Two‐year results from a randomized controlled trial. Journal of Bone and Mineral Research 2014;29(6):1346‐55. - PubMed
- Staples MP, Howe BM, Ringler M, Mitchell P, Wriedt C, Wark J, et al. Vertebroplasty for osteoporotic vertebral fractures: radiological outcomes from a 2 year randomized controlled trial. Archives of Osteoporosis 2015;10(1):229. - PMC - PubMed
-
- Chen D, An ZQ, Song S, Tang JF, Qin H. Percutaneous vertebroplasty compared with conservative treatment in patients with chronic painful osteoporotic spinal fractures. Journal of Clinical Neuroscience 2014;21:473‐7. - PubMed
-
- Bird P, Clark W, Diamond T, Schlaphoff G, Smerdely P, Gonski P, et al. A placebo controlled trial of vertebral fill technique vertebroplasty for acute painful osteoporotic fracture (VAPOUR trial). Arthritis and Rheumatology. Conference: American College of Rheumatology/Association of Rheumatology Health Professionals Annual Scientific Meeting. 2016; Vol. 68:413‐4.
- Clark W, Bird P, Diamond T, Gonski P. Vertebroplasty for acute painful osteoporotic fractures (VAPOUR): study protocol for a randomized controlled trial. Trials 2015;16:159. - PMC - PubMed
- Clark W, Bird P, Gonski P, Diamond T, Smerdely P, McNeil H, et al. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicentre, randomised, double‐blind, placebo‐controlled trial. Lancet 2016;388(10052):1408‐16. - PubMed
References to studies excluded from this review
-
- Cai J, Hao YW, Li C, Yang HQ. Percutaneous vertebroplasty with bone cement injection for osteoporotic vertebral compression fractures via transpedicular approach [Chinese]. Chinese Journal of Tissue Engineering Research 2015;19(30):4892‐7.
-
- Chen C, Bian J, Zhang W, Zhao C, Wei H. Unilateral versus bilateral vertebroplasty for severe osteoporotic vertebral compression fractures. Journal of Spinal Disorders & Techniques 2014;27(8):E301‐4. - PubMed
-
- Chen‐lei L, Yi‐he H, Gui‐qing W, Yong‐zhi T, Xiang‐jiang W, Han‐tao H. Curative effects of unipedicular and bipedicular vertebroplasty in treating osteoporotic vertebral compression fractures in the elderly population. Journal of Xi'an Jiatong University 2015;36:6.
-
- Du J, Li X, Lin X. Kyphoplasty versus vertebroplasty in the treatment of painful osteoporotic vertebral compression fractures: two‐year follow‐up in a prospective controlled study. Acta Orthopaedica Belgica 2014;80(4):477‐86. - PubMed
References to studies awaiting assessment
-
- Chen JP, Qi XW, Li SJ, Kuang LP, Yuan XH, Wang GS, et al. Bone cement injection as vertebral augmentation therapy for osteoporotic vertebral compression fractures. [Chinese]. Chinese Journal of Tissue Engineering Research 2015;19(21):3292‐6. [DOI: 10.3969/j.issn.2095-4344.2015.21.003] - DOI
-
- Doin S. A randomised controlled trial of vertebroplasty for the treatment of osteoporotic vertebral crush fractures. http://www.isrctn.com/ISRCTN14442024 (first received 12 September 2003) Trial completed.
-
- NCT00749060. Prospective randomized comparative study of balloon kyphoplasty, vertebroplasty and conservative management in acute osteoporotic vertebral fractures of less than 6 weeks. clinicaltrials.gov/show/NCT00749060 (first received September 8, 2008) Trial completed June 2012.
-
- NCT00749086. Prospective randomized study of balloon kyphoplasty and vertebroplasty in subacute (older than 6 weeks) osteoporotic vertebral fractures (STIC2). clinicaltrials.gov/show/NCT00749086 Trial registered: NCT00749086. Recruitment commenced Dec 2007. Trial completed June 2012.
-
- Li DH, Liu XW, Peng XT, Wang ZG, Wang BC, Jin P, et al. Bone filling mesh container for treatment of vertebral compression fractures can reduce the leakage of bone cement. [Chinese]. Chinese Journal of Tissue Engineering Research 15 Jan 2015;19(3):358‐3.
References to ongoing studies
-
- Longo UG, Loppini M, Denaro L, Brandi ML, Maffulli N, Denaro V. The effectiveness and safety of vertebroplasty for osteoporotic vertebral compression fractures. A double blind, prospective, randomized, controlled study. Clinical Cases in Mineral and Bone Metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases 2010;7(2):109‐13. [PUBMED: 22460014] - PMC - PubMed
-
- NCT01677806. Investigational percutaneous vertebroplasty efficacy and safety trial. clinicaltrials.gov/show/NCT01677806 (first received 23 August 2012).
-
- NCT01963039. A trial of vertebroplasty for painful chronic osteoporotic vertebral fractures (VERTOS V). clinicaltrials.gov/show/NCT01963039 First registered 28 August 2013.
Additional references
-
- Anderson PA, Froyshteter AB, Tontz WL Jr. Meta‐analysis of vertebral augmentation compared with conservative treatment for osteoporotic spinal fractures. Journal of Bone and Mineral Research 2013;28(2):378‐32. - PubMed
-
- Baumann A, Tauss J, Baumann G, Tomka M, Hessinger M, Tiesenhausen K. Cement embolization into the vena cava and pulmonal arteries after vertebroplasty: interdisciplinary management. European Journal of Vascular and Endovascular Surgery 2006;31(5):558‐61. - PubMed
-
- Belkoff S, Mathis JM, Jasper LE, Deramond H. The biomechanics of vertebroplasty: The effect of cement volume on mechanical behavior. Spine 2001;26(14):1537‐41. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical