

Filaria specific antibody response profiling in plasma from anti-retroviral naïve Loa loa microfilaraemic HIV-1 infected people
- PMID: 29618330
- PMCID: PMC5885382
- DOI: 10.1186/s12879-018-3072-2
Filaria specific antibody response profiling in plasma from anti-retroviral naïve Loa loa microfilaraemic HIV-1 infected people
Abstract
Background: In West and Central Africa areas of endemic Loa loa infections overlap with regions of high prevalence of human immunodeficiency virus type 1 (HIV-1) infections. Because individuals in this region are exposed to filarial parasites from birth, most HIV-1 infected individuals invariably also have a history of filarial parasite infection. Since HIV-1 infection both depletes immune system and maintains it in perpetual inflammation, this can hamper Loa loa filarial parasite mediated immune modulation, leading to enhanced loaisis.
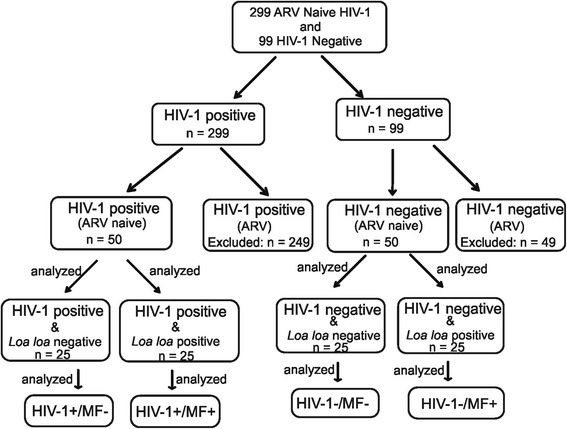
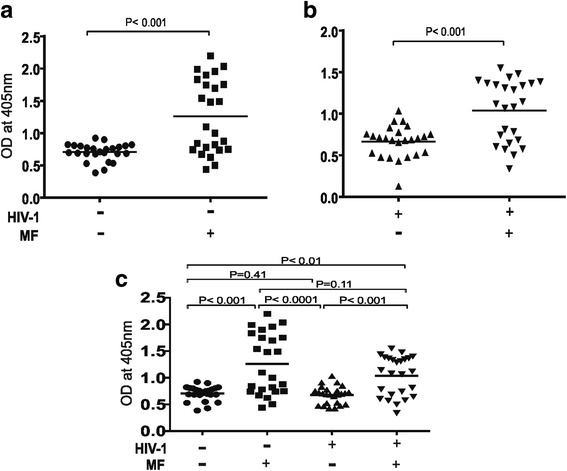
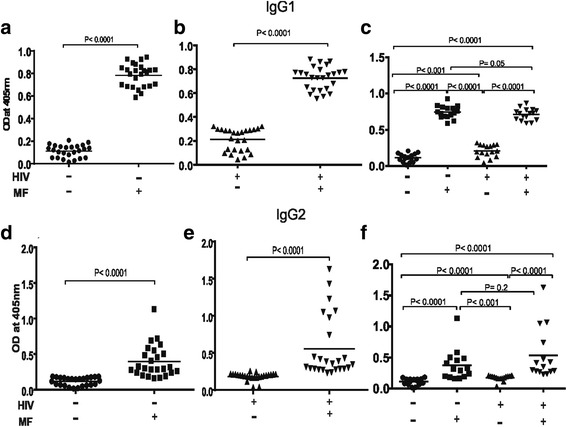
Methods: In this study we have assessed in plasma from asymptomatic anti-retroviral (ARV) naïve Loa loa microfilaraemic HIV-1 infected people the filarial antibody responses specific to a filariasis composite antigen consisting of Wbgp29-BmR1-BmM14-WbSXP. The antibody responses specific to the filariasis composite antigen was determined by enzyme linked immunosorbent assay (ELISA) in plasma from ARV naïve Loa loa microfilaraemic HIV-1 infected participants. In addition the filarial antigen specific IgG antibody subclass profiles were also determined for both HIV-1 positive and negative people.
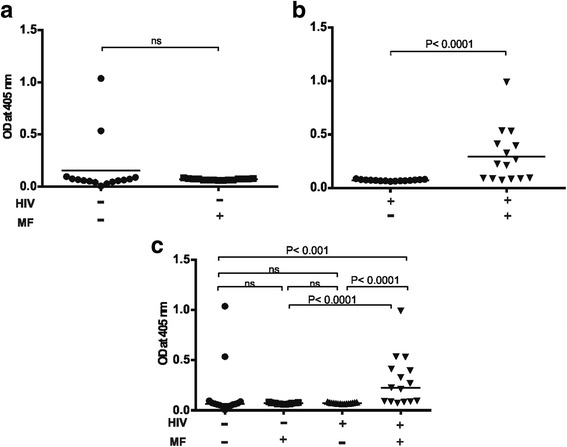
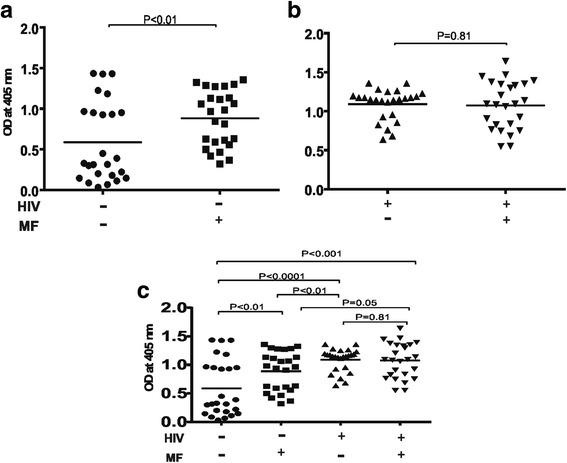
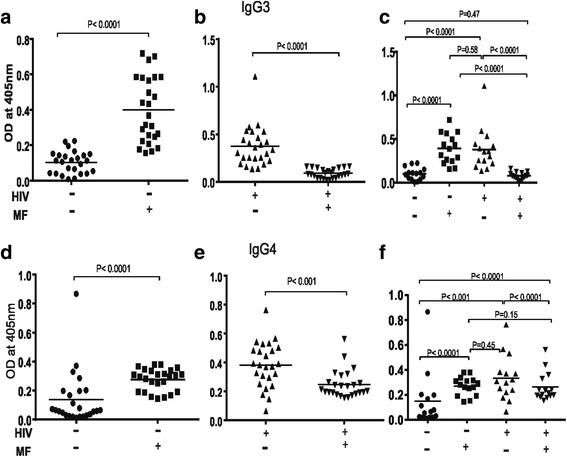
Results: Both Loa loa microfilaraemic HIV-1 positive and negative individuals showed significantly higher plasma levels of IgG1 (P < 0.0001), IgG2 (P < 0.0001) and IgM (P < 0.0001) relative to amicrofilaraemic participants. A significant increase in IgE (P < 0.0001) was observed exclusively in Loa loa microfilaraemic HIV-1 infected people. In contrast there was a significant reduction in the level of IgG4 (p < 0.0001) and IgG3 (P < 0.0001) in Loa loa microfilaraemic HIV-1 infected individuals.
Conclusions: Loa loa microfilaraemia in ARV naïve HIV-1 infected people through differential reduction of plasma levels of filarial antigen specific IgG3, IgG4 and a significant increase in plasma levels of filarial antigen specific IgE could diminish Loa loa mediated immune-regulation. This in effect can result to increase loaisis mediated immunopathology in antiretroviral naive HIV-1 infected people.
Keywords: African eye worm; HIV-1; Loa loa; Loaisis; Microfilaraemia.
Conflict of interest statement
Ethics approval and consent to participate
All human samples in the AFRODEC Cohort were collected with written informed consent under clinical protocols approved by the Republic of Cameroon National Ethics Committee (protocol number 2014/10/499/CE/CNERSH/SP) the CIRCB institutional review board (protocol number 14-11) and the Cameroon government administrative authorization (authorization number 631-1112). The AFRODEC cohort consists of adult HIV-1 infected participants aged 21 to 65 years who were naïve to antiretroviral therapy.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Zoure HG, Wanji S, Noma M, Amazigo UV, Diggle PJ, Tekle AH, et al. The geographic distribution of Loa loa in Africa: results of large-scale implementation of the rapid assessment procedure for Loiasis (RAPLOA) PLoS Negl Trop Dis. 2011;5(6):e1210. doi: 10.1371/journal.pntd.0001210. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
