

Efficacy of virtual block objects in reducing the lung dose in helical tomotherapy planning for cervical oesophageal cancer: a planning study
- PMID: 29618353
- PMCID: PMC5885420
- DOI: 10.1186/s13014-018-1012-3
Efficacy of virtual block objects in reducing the lung dose in helical tomotherapy planning for cervical oesophageal cancer: a planning study
Abstract
Background: Intensity-modulated radiotherapy is useful for cervical oesophageal carcinoma (CEC); however, increasing low-dose exposure to the lung may lead to radiation pneumonitis. Nevertheless, an irradiation technique that avoids the lungs has never been examined due to the high difficulty of dose optimization. In this study, we examined the efficacy of helical tomotherapy that can restrict beamlets passing virtual blocks during dose optimization computing (block plan) in reducing the lung dose.
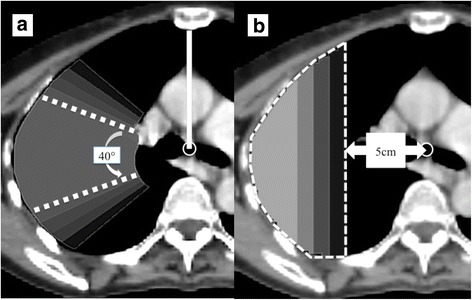
Methods: Fifteen patients with CEC were analysed. The primary/nodal lesion and prophylactic nodal region with adequate margins were defined as the planning target volume (PTV)-60 Gy and PTV-48 Gy, respectively. Nineteen plans per patient were made and compared (total: 285 plans), including non-block and block plans with several shapes and sizes.
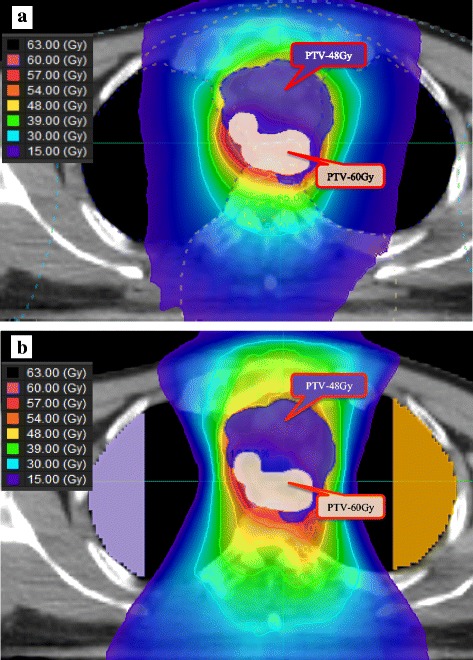
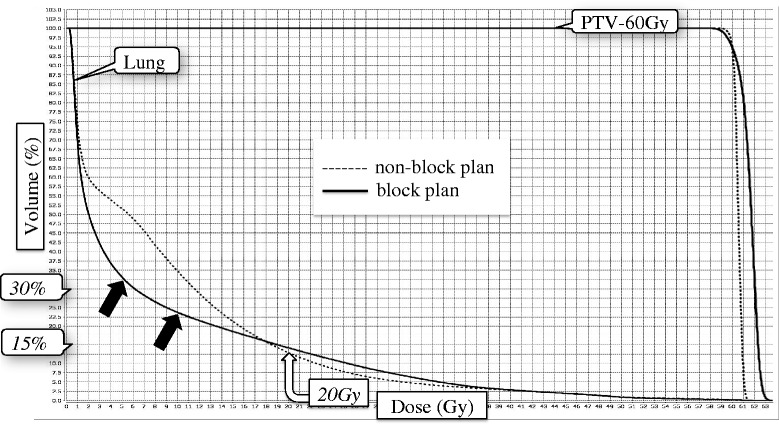
Results: The most appropriate block model was semi-circular, 8 cm outside of the tracheal bifurcation, with a significantly lower lung dose compared to that of non-block plans; the mean lung volumes receiving 5 Gy, 10 Gy, 20 Gy, and the mean lung dose were 31.3% vs. 48.0% (p < 0.001), 22.4% vs. 39.4% (p < 0.001), 13.2% vs. 16.0% (p = 0.028), and 7.1 Gy vs. 9.6 Gy (p < 0.001), respectively. Both the block and non-block plans were comparable in terms of the homogeneity and conformity indexes of PTV-60 Gy: 0.05 vs. 0.04 (p = 0.100) and 0.82 vs. 0.85 (p = 0.616), respectively. The maximum dose of the spinal cord planning risk volume increased slightly (49.4 Gy vs. 47.9 Gy, p = 0.002). There was no significant difference in the mean doses to the heart and the thyroid gland. Prolongation of the delivery time was less than 1 min (5.6 min vs. 4.9 min, p = 0.010).
Conclusions: The block plan for CEC could significantly reduce the lung dose, with acceptable increment in the spinal dose and a slightly prolonged delivery time.
Keywords: Cervical oesophageal cancer; Complete block; Directional block; Helical tomotherapy; Intensity-modulated radiation therapy; Lung dose.
Conflict of interest statement
Ethics approval and consent to participate
All procedures involving human participants were in accordance with the ethical standards of the institutional research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
All patients gave written informed consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Tachimori Y, Ozawa S, Numasaki H, Fujishiro M, Matsubara H, Oyama T, Shinoda M, Toh Y, Udagawa H, Uno T. Registration Committee for Esophageal Cancer of the Japan esophageal S: comprehensive registry of esophageal Cancer in Japan, 2009. Esophagus. 2016;13:110–137. doi: 10.1007/s10388-016-0531-y. - DOI - PMC - PubMed
-
- Zenda S, Kojima T, Kato K, Izumi S, Ozawa T, Kiyota N, Katada C, Tsushima T, Ito Y, Akimoto T, et al. Multicenter phase 2 study of Cisplatin and 5-fluorouracil with concurrent radiation therapy as an organ preservation approach in patients with Squamous cell carcinoma of the cervical esophagus. Int J Radiat Oncol Biol Phys. 2016;96:976–984. doi: 10.1016/j.ijrobp.2016.08.045. - DOI - PubMed
-
- McDowell LJ, Huang SH, Xu W, Che J, RKS W, Brierley J, Kim J, Cummings B, Waldron J, Bayley A, et al. Effect of intensity modulated radiation therapy with concurrent chemotherapy on survival for patients with cervical esophageal carcinoma. Int J Radiat Oncol Biol Phys. 2017;98:186–195. doi: 10.1016/j.ijrobp.2017.01.003. - DOI - PubMed
-
- Cao CN, Luo JW, Gao L, Xu GZ, Yi JL, Huang XD, Wang K, Zhang SP, Qu Y, Li SY, et al. Intensity-modulated radiotherapy for cervical esophageal squamous cell carcinoma: clinical outcomes and patterns of failure. Eur Arch Otorhinolaryngol. 2016;273:741–747. doi: 10.1007/s00405-015-3576-y. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
