

Bisphosphonate therapy for spinal osteoporosis in Hajdu-Cheney syndrome - new data and literature review
- PMID: 29618366
- PMCID: PMC5885380
- DOI: 10.1186/s13023-018-0795-5
Bisphosphonate therapy for spinal osteoporosis in Hajdu-Cheney syndrome - new data and literature review
Erratum in
-
Correction to: Bisphosphonate therapy for spinal osteoporosis in Hajdu-Cheney syndrome - new data and literature review.Orphanet J Rare Dis. 2019 May 10;14(1):104. doi: 10.1186/s13023-019-1084-7. Orphanet J Rare Dis. 2019. PMID: 31077240 Free PMC article.
Abstract
Background: Hajdu-Cheney syndrome (HCS) (#OMIM 102500) is a rare, autosomal dominant condition that presents in early childhood. It is caused by mutations in the terminal exon of NOTCH2, which encodes the transmembrane NOTCH2 receptor. This pathway is involved in the coupled processes of bone formation and resorption. The skeletal features of HCS include acro-osteolysis of the digits and osteoporosis commonly affecting vertebrae and long bones. Fractures are a prominent feature and are associated with significant morbidity. There is no specific treatment, but with both acro-osteolysis and generalized osteoporosis, it is possible that anti-resorptive treatment might be of benefit. However, to date only a few case reports have evaluated the effectiveness of bisphosphonate treatment.
Methods: We describe the clinical features, treatment regimens and response to bisphosphonate treatment in 7 newly described patients aged 6-39 with HCS, and pooled the data with that from 8 previously published cases (a total of 17 courses of treatment in 15 individuals).
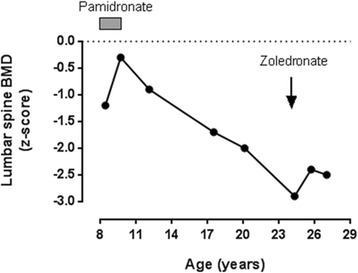
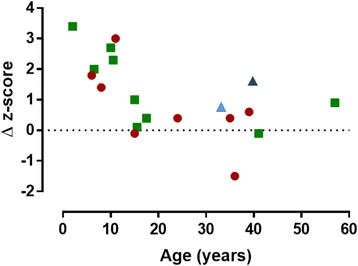
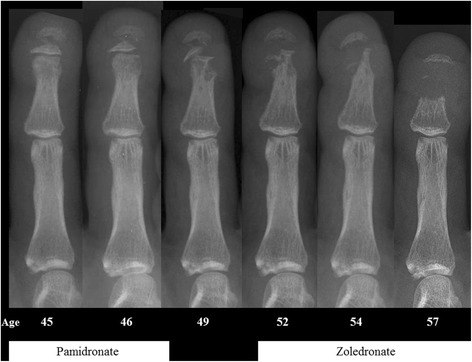
Results: The mean lumbar spine bone mineral density (BMD) z-score before treatment was - 2.9 (SD 1.2). In 14 courses of treatment (82%), there was an increase in BMD with bisphosphonate treatment, but the impact (in terms of change in spinal BMD z-score) appeared to be less with advancing age (p = 0.01). There was no evidence that acro-osteolysis was prevented.
Conclusions: Although individual response is variable and age-related, the data support a role for bisphosphonates in preventing or treating spinal osteoporosis in HCS, but bone loss from the lumbar spine may be rapid after cessation.
Keywords: Bisphosphonates; Diseases; Dual energy x-ray absorptiometry (DEXA); Genetic disorders; Human studies.
Conflict of interest statement
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Consent for publication
Not applicable
Competing interests
Dr. Rhee reports personal fees from Amgen, personal fees from Eli Lilly, outside the submitted work. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Cheney WD. Acro-Osteolysis. Am J Roentgenol Radium Therapy Nucl Med. 1965;94:595–607. - PubMed
-
- Albano LM, Bertola DR, Barba MF, Valente M, Robertson SP, Kim CA. Phenotypic overlap in Melnick-needles, serpentine fibula-polycystic kidney and Hajdu-Cheney syndromes: a clinical and molecular study in three patients. Clin Dysmorphol. 2007;16(1):27–33. doi: 10.1097/01.mcd.0000228418.74413.52. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
