

Aromatase inhibitors are associated with a higher fracture risk than tamoxifen: a systematic review and meta-analysis
- PMID: 29619093
- PMCID: PMC5871065
- DOI: 10.1177/1759720X18759291
Aromatase inhibitors are associated with a higher fracture risk than tamoxifen: a systematic review and meta-analysis
Abstract
Background: In this paper, our aim was to systematically evaluate published evidence of bone fracture risk associated with tamoxifen and aromatase inhibitors in women aged 65 and under, and diagnosed with nonmetastatic breast cancer.
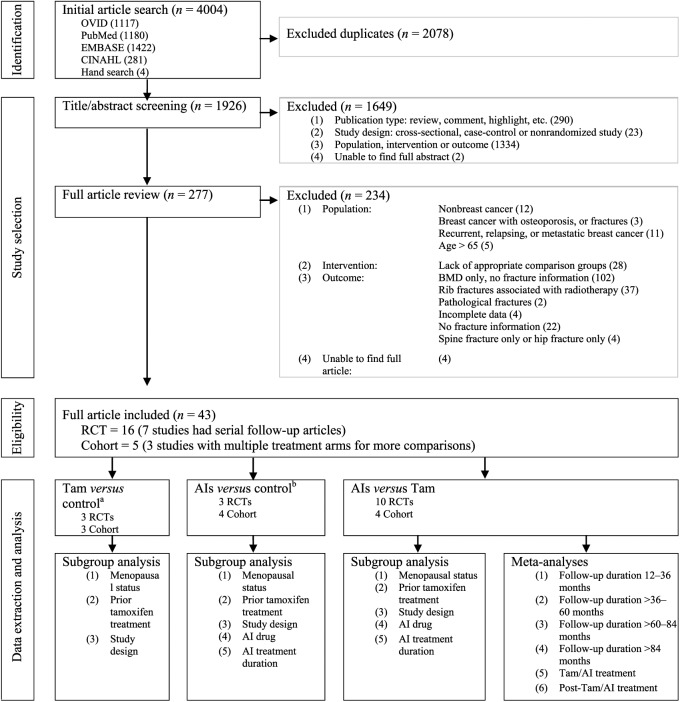
Methods: We comprehensively searched MEDLINE, EMBASE and CINAHL databases from January 1997 through May 2015, and reference lists of the selected articles to identify English-language randomized controlled trials and cohort studies of fracture risk. Two independent reviewers screened articles and assessed methodological quality using Risk of Bias assessment for randomized controlled trials and the Newcastle-Ottawa Scale for cohort studies. Fracture risk was estimated as pooled risk ratios using a random-effects model and inverse variance method.
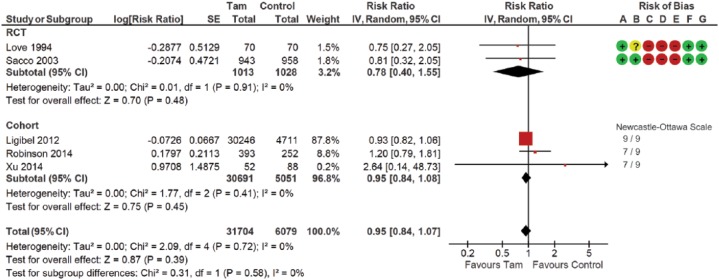
Results: Of 1926 identified articles, 21 independent studies fulfilled our selection criteria. Similar fracture risk was observed in women treated and not treated with tamoxifen [pooled risk ratio (RR) 0.95; 95% confidence interval (CI) 0.84-1.07]. A 35% (95% CI 1.21-1.51) higher fracture risk was observed in the aromatase inhibitor group compared with the tamoxifen group. A 17% (95% CI 1.07-1.28) higher fracture risk was observed in the aromatase inhibitor group than the no aromatase inhibitor group. Compared with the tamoxifen group, aromatase inhibitor-associated fracture risk increased by 33% (pooled RR 1.33; 95% CI 1.21-1.47) during the tamoxifen/aromatase inhibitor treatment period, but did not increase (pooled RR 0.99; 95% CI 0.72-1.37) during the post-tamoxifen/aromatase inhibitor treatment period.
Conclusions: Fracture risk is significantly higher in women treated with aromatase inhibitors, especially during the treatment period. Tamoxifen is not associated with lower fracture risk while tamoxifen could potentially preserve bone mass. Better osteoporosis management programs, especially during the treatment period, are needed for this group of women.
Keywords: aromatase inhibitors; breast cancer; fracture risk; hormonal treatment; tamoxifen; women.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
 Low risk of bias
Low risk of bias  Unknown risk of bias
Unknown risk of bias  High risk of bias CI, confidence interval; d.f., degrees of freedom; IV, inverse variance; RCT, randomized controlled trial; SE, standard error; Tam, tamoxifen.
High risk of bias CI, confidence interval; d.f., degrees of freedom; IV, inverse variance; RCT, randomized controlled trial; SE, standard error; Tam, tamoxifen.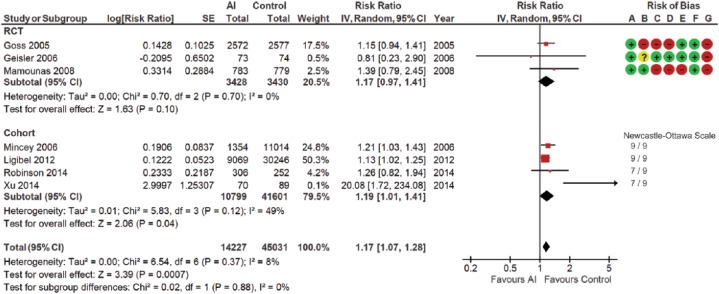 Low risk of bias Unknown risk of bias High risk of bias AI, aromatase inhibitor; CI, confidence interval; d.f., degrees of freedom; IV, inverse variance; RCT, randomized controlled trial; SE, standard error.
Low risk of bias Unknown risk of bias High risk of bias AI, aromatase inhibitor; CI, confidence interval; d.f., degrees of freedom; IV, inverse variance; RCT, randomized controlled trial; SE, standard error.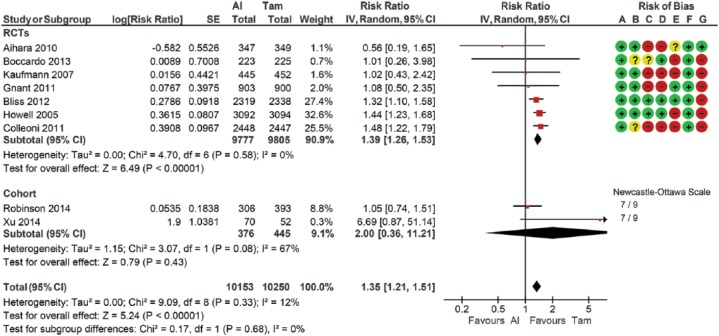 Low risk of bias Unknown risk of bias High risk of bias AI, aromatase inhibitor; CI, confidence interval; IV, inverse variance; RCT, randomized controlled trial; SE, standard error; Tam, tamoxifen.
Low risk of bias Unknown risk of bias High risk of bias AI, aromatase inhibitor; CI, confidence interval; IV, inverse variance; RCT, randomized controlled trial; SE, standard error; Tam, tamoxifen.References
-
- Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med 2005; 353: 1784–1792. - PubMed
-
- Goldhirsch A, Wood WC, Gelber RD, et al. Meeting highlights: updated international expert consensus on the primary therapy of early breast cancer. J Clin Oncol 2003; 21: 3357–3365. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
