

Daikenchuto for reducing postoperative ileus in patients undergoing elective abdominal surgery
- PMID: 29619778
- PMCID: PMC6494569
- DOI: 10.1002/14651858.CD012271.pub2
Daikenchuto for reducing postoperative ileus in patients undergoing elective abdominal surgery
Retraction in
-
Daikenchuto for reducing postoperative ileus in patients undergoing elective abdominal surgery.Cochrane Database Syst Rev. 2020 Mar 25;3(3):CD012271. doi: 10.1002/14651858.CD012271.pub3. Cochrane Database Syst Rev. 2020. PMID: 32212387 Free PMC article. Review.
Abstract
Background: Postoperative ileus is a major complication for persons undergoing abdominal surgery. Daikenchuto, a Japanese traditional medicine (Kampo), is a drug that may reduce postoperative ileus.
Objectives: To assess the efficacy and safety of Daikenchuto for reducing prolonged postoperative ileus in persons undergoing elective abdominal surgery.
Search methods: We searched the following databases on 3 July 2017: CENTRAL, MEDLINE, Embase, ICHUSHI, WHO (World Health Organization) International Clinical Trials Registry Platform (ICTRP), EU Crinical Trials registry (EU-CTR), UMIN Clinical Trials Registry (UMIN-CTR), ClinicalTrials.gov, The Japan Society for Oriental Medicine (JSOM), American Society of Clinical Oncology (ASCO), Society of American Gastrointestinal and Endscopic Surgeons (SAGES). We set no limitations on language or date of publication.
Selection criteria: We included randomised controlled trials (RCTs) comparing Daikenchuto with any control condition in adults, 18 years of age or older, undergoing elective abdominal surgery.
Data collection and analysis: We applied standard methodological procedures expected by Cochrane. Two review authors independently reviewed the articles identified by literature searches, extracted data, and assessed risk of bias of the included studies using the Cochrane software Review Manager 5.
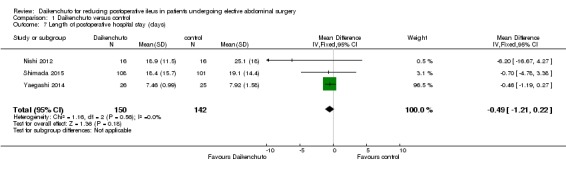
Main results: We included seven RCTs with a total of 1202 participants. Overall, we judged the risk of bias as low in four studies and high in three studies. We are uncertain whether Daikenchuto reduced time to first flatus (mean difference (MD) -11.32 hours, 95% confidence interval (CI) -17.45 to -5.19; two RCTs, 83 participants; very low-quality evidence), or time to first bowel movement (MD -9.44 hours, 95% CI -22.22 to 3.35; four RCTs, 500 participants; very low-quality evidence) following surgery. There was little or no difference in time to resumption of regular solid food following surgery (MD 3.64 hours, 95% CI -24.45 to 31.74; two RCTs, 258 participants; low-quality evidence). There were no adverse events in either arm of the five RCTs that reported on drug-related adverse events (risk difference (RD) 0.00, 95% CI -0.02 to 0.02, 568 participants, low-quality evidence). We are uncertain of the effect of Daikenchuto on patient satisfaction (MD 0.09, 95% CI -0.19 to 0.37; one RCT, 81 participants; very low-quality of evidence). There was little or no difference in the incidence of any re-interventions for postoperative ileus before leaving hospital (risk ratio (RR) 0.99, 95% CI 0.06 to 15.62; one RCT, 207 participants; moderate-quality evidence), or length of hospital stay (MD -0.49 days, 95% CI -1.21 to 0.22; three RCTs, 292 participants; low-quality evidence).
Authors' conclusions: Evidence from current literature was unclear whether Daikenchuto reduced postoperative ileus in patients undergoing elective abdominal surgery, due to the small number of participants in the meta-analyses. Very low-quality evidence means we are uncertain whether Daikenchuto improved postoperative flatus or bowel movement. Further well-designed and adequately powered studies are needed to assess the efficacy of Daikenchuto.
Conflict of interest statement
Nobuaki Hoshino has received writing fees from Igaku‐Shoin and Kanehara publishers.
Suguru Hasegawa has received lecture fees from Olympus, Johnson & Johnson, Covidien Japan, Stryker, Chugai, Taiho, Yakult. He has received grant or research support from the Japanese Ministry of Education, Culture, Sports, Science and Technology, and Taiho.
Toshihiko Takada has received a grant from St. Luke's Life Science Institute.
Koya Hida has received grants for research about the treatment of rectal cancer from the Japanese Society of Clinical Oncology, The Japanese Foundation for Research and Promotion of Endoscopy. He has received writing fees from the Medical View Company and the Nanko‐do Company.
Toshi A Furukawa has received lecture fees from Eli Lilly, Janssen, Meiji, Mitsubishi‐Tanabe, MSD, and Pfizer and consultancy fees from the Takeda Science Foundation. He has received royalties from Igaku‐Shoin and Nihon Bunka Kagaku‐sha publishers. He has received research support from Mochida and Mitsubishi‐Tanabe.
Yoshiharu Sakai has received lecture fees from Olympus, Johnson & Johnson, Covidien Japan, Stryker, Chugai, Taiho, Yakult, Takeda, Terumo. He has received grant or research support from the Japanese Ministry of Education, Culture, Sports, Science and Technology, Tsumura, Daiichisankyo, Taiho, Chugai, Yakult, Shionogi, Otsuka and Sanofi.
Figures










References
References to studies included in this review
-
- Akamaru Y, Takahashi T, Nishida T, Omori T, Nishikawa K, Mikata S, et al. Effects of Daikenchuto, a Japanese herb, on intestinal motility after total gastrectomy: a prospective randomized trial. Journal of Gastrointestinal Surgery 2015;19:467‐72. - PubMed
-
- Katsuno H, Maeda K, Kaiho T, Kunieda K, Funabashi K, Sakamoto J, et al. Clinical efficacy of Daikenchuto for gastrointestinal dysfunction following colon surgery: a randomized, double‐blind, multicenter, placebo‐controlled study. Japanese Journal of Clinical Oncology 2015;45:650‐6. [JFMC39‐0902] - PMC - PubMed
- Katsuno H, Maeda K, Ohya M, Yoshioka K, Tsunoda A, Koda K, et al. Clinical pharmacology of Daikenchuto assessed by transit analysis using radiopaque markers in patients with colon cancer undergoing open surgery: a multicenter double‐blind randomized placebo‐controlled study. Journal of Gastroenterology 2016;51:222‐9. [JFMC39‐0902 additional study] - PubMed
-
- Nishi M, Shimada M, Uchiyama H, Ikegami T, Arakawa Y, Hanaoka J, et al. The beneficial effects of Kampo medicine Dai‐ken‐chu‐to after hepatic resection: a prospective randomized control study. Hepato‐Gastroenterology 2012;59:2990‐4. - PubMed
-
- Okada K‐i, Kawai M, Hirono S, Fujii T, Kodera Y, Sho M, et al. Evaluation of the efficacy of Daikenchuto (TJ‐100) for the prevention of paralytic ileus after pancreaticoduodenectomy: a multicenter, double‐blind, randomized, placebo‐controlled trial. Surgery 2016;159:1333‐41. - PubMed
-
- Shimada M, Morine Y, Nagano H, Hatano E, Kaiho T, Miyazaki M, et al. Effect of TU‐100, a traditional Japanese medicine, administered after hepatic resection in patients with liver cancer: a multicenter, phase III trial. International Journal of Clinical Oncology 2015;20:95‐104. [JFMC40‐1001] - PubMed
References to studies excluded from this review
-
- Fujii S. The effect of Daikenchutou on early gut motility after colorectal cancer operation [大腸癌術後早期腸管運動における大建中湯の効果]. Progress in Medicine 2011;31:468‐9.
-
- Kaiho T, Tanaka T, Tsuchiya S, Yanagisawa S, Takeuchi O, Miura M, et al. Effect of the herbal medicine Dai‐kenchu‐to for serum ammonia in hepatectomised patients. Hepato‐Gastroenterology 2004;52:161‐5. - PubMed
-
- Kaiho T, Shinmura K, Nishimura M, Fujimoto T. Effectiveness of perioperative management of hepatectomised patients in biliary disease with Japanese Kampo medicine in terms of residual liver circulation [胆道疾患肝切除時における漢方製剤を用いた周術期管理の有用性]. Journal of Japan Biliary Association 2015;29:206‐13.
-
- Naka S, Yanagie H, Yasuhara H. Improvement effect of traditional Chinese medicinal supplement on nitrogen metabolism after surgery and cytokine dynamics [手術後窒素代謝およびサイトカイン動態に対する漢方補剤の改善効果]. Progress in Medicine 2002;22:1360‐1.
-
- Osawa G, Yoshimatsu K, Yokomizo H, Otani T, Matsumoto A, Nakayama M, et al. The clinical effects of Dai‐kenchu‐to on postoperative intestinal movement and inflammatory reaction in colorectal surgery. Hepato‐Gastroenterology 2015;62:807‐10. - PubMed
References to ongoing studies
-
- Akamatsu H. Clinical effectiveness of daikenchuto (TJ‐100) on gastrointestinal symptom after colectomy in colorectal cancer patients with abdominal pain and distention due to a bowel movement disorder [腹痛,腹部膨満感を有する便通障害患者における大腸癌手術後の腹痛,腹部膨満感等の消化器症状に対する大建中湯(TJ‐100)の臨床的効果の検討]. UMIN Clinical Trials Registry 2012;UMIN000008348.
-
- Eguchi T. Exploratory study of daikenchuto for nutritional management following colectomy of colon cancer [大腸癌術後の栄養管理法についての検討~大建中湯の探索的検討~]. UMIN Clinical Trials Registry 2011;UMIN000006413.
-
- Jensen C. Effect of TU‐100 in patients undergoing laparoscopic colectomy (TU100P2T3). ClinicalTrials.gov 2014;NCT02232893.
-
- Kaido T. Randomized controlled trial of Japanese herbal medicine, daikenchuto for preventive effects of bowel dysfunction after adult liver transplantation [成人肝臓移植術後の消化管障害に対するTJ‐100ツムラ大建中湯(医療用)の有効性に関する検討 ‐多施設共同による二重盲検無作為化比較臨床試験‐]. UMIN Clinical Trials Registry 2014;UMIN000014326.
-
- Mochida S. A tolerability and efficacy study of TU‐100 for the treatment of postoperative ileus. ClinicalTrials.gov 2005;NCT00266461.
Additional references
-
- Behm B, Stollman N. Postoperative ileus: etiologies and interventions. Clinical Gastroenterology and Hepatology 2003;1(2):71‐80. - PubMed
-
- Ehlers AP, Simianu VV, Bastawrous AL, Billingham RP, Davidson GH, Fichera A, et al. Alvimopan use, outcomes, and costs: a report from the surgical care and outcomes assessment program comparative effectiveness research translation network collaborative. Journal of the American College of Surgeons 2016;222:870‐7. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous