

A systematic review and meta-analysis of single-incision mini-slings (MiniArc) versus transobturator mid-urethral slings in surgical management of female stress urinary incontinence
- PMID: 29620645
- PMCID: PMC5902257
- DOI: 10.1097/MD.0000000000010283
A systematic review and meta-analysis of single-incision mini-slings (MiniArc) versus transobturator mid-urethral slings in surgical management of female stress urinary incontinence
Abstract
Background: To assess the current evidence of effectiveness and safety of single-incision mini-slings (MiniArc) versus transobturator midurethral slings in the management of female stress urinary incontinence (SUI).
Methods: A systematic search was performed from the electronic databases including PubMed, EMBASE, and Cochrane Library by November 2017. Using RevMan5.3 statistical software, the primary outcomes including subject and objective cure rates at 6 to 24 months follow-up were evaluated. Meanwhile, analysis was also performed for comparing the secondary outcomes such as peri- and postoperative complications, operative data, and quality of life.
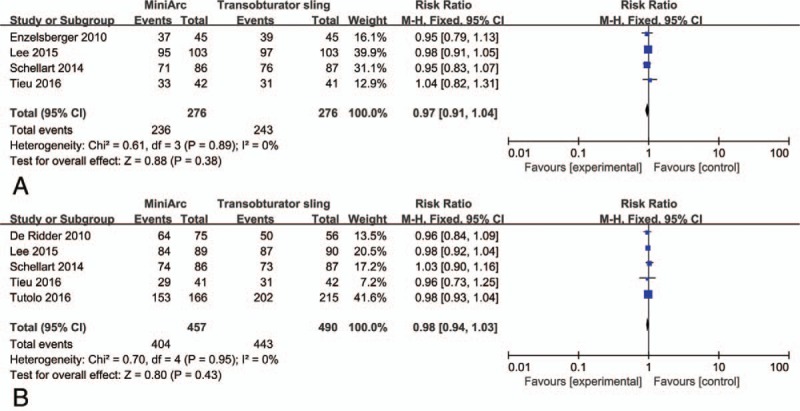
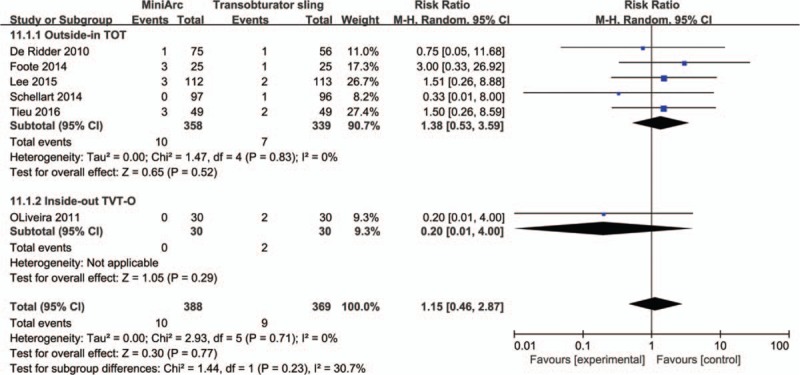
Results: Six randomized controlled trials (RCTs) and 6 retrospective cohort studies involving 1794 patients with SUI were analyzed based on the inclusion criteria. On the basis of our analysis, MiniArc was proven to have a noninferior clinical efficacy compared with transobturator midurethral slings with respect to the objective cure rate (risk ratio [RR] = 0.98, 95% confidence interval [CI] 0.94-1.03, P = .43) and subjective cure rate (RR = 0.97, 95% CI 0.91-1. 04, P = .38). In addition, pooled analysis showed that MiniArc had significantly lower postoperative pain scores (mean difference [MD] = -1.70, 95% CI -3.17 to -0.23, P = .02) and less postoperative groin pain (RR = 0.42, 95% CI 0.18-0.98, P = .04). Moreover, the MiniArc group also had a significantly shorter operation time (MD = -6.12, 95% CI -8.61 to -3.64, P < .001), less blood loss (MD = -16.67, 95% CI -26.29 to -7.05, P < .001), shorter in-patient stay (MD = 1.30, 95% CI -1.74 to -0.86, P < .001), and less urinary retention risk (RR = 1.15, 95% CI 0.46-2.87, P = .77). However, overall evidence was insufficient to suggest a statistically significant difference in the adverse event profile for MiniArc compared with transobturator slings.
Conclusions: This meta-analysis indicates that MiniArc is an effective method treating SUI. When compared with transobturator slings, it not only has a similar high cure rates, but also is associated with shorter operation time, less blood loss, more favorable recovery time, lower postoperative pain scores, less postoperative groin pain, less urinary retention, and absence of a visible wound. However, the findings of this study should be further confirmed by well-designed prospective RCTs with a larger patient series.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures












References
-
- Maral I, Ozkardeş H, Peşkircioğlu L, et al. Prevalence of stress urinary incontinence in both sexes at or after age 15 years: a cross-sectional study. J Urol 2001;165:408–12. - PubMed
-
- Nambiar A, Cody JD, Jeffery ST. Single-incision sling operations for urinary incontinence in women. Cochrane Database Syst Rev 2014;7:CD008709. - PubMed
-
- Mostafa A, Agur W, Abdel-All M, et al. A multicentre prospective randomised study of single-incision mini-sling (Ajust®) versus tension-free vaginal tape-obturator (TVT-O™) in the management of female stress urinary incontinence: pain profile and short-term outcomes. Eur J Obstet Gynecol Reprod Biol 2012;165:115–21. - PubMed
-
- Beyar N, Groutz A. Pelvic floor muscle training for female stress urinary incontinence: five years outcomes. Neurourol Urodyn 2017;36:132–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
