

Long-term Accuracy of Breast Cancer Risk Assessment Combining Classic Risk Factors and Breast Density
- PMID: 29621362
- PMCID: PMC6143016
- DOI: 10.1001/jamaoncol.2018.0174
Long-term Accuracy of Breast Cancer Risk Assessment Combining Classic Risk Factors and Breast Density
Abstract
Importance: Accurate long-term breast cancer risk assessment for women attending routine screening could help reduce the disease burden and intervention-associated harms by personalizing screening recommendations and preventive interventions.
Objective: To report the accuracy of risk assessment for breast cancer during a period of 19 years.
Design, setting, and participants: This cohort study of the Kaiser Permanente Washington breast imaging registry included women without previous breast cancer, aged 40 to 73 years, who attended screening from January 1, 1996, through December 31, 2013. Follow-up was completed on December 31, 2014, and data were analyzed from March 2, 2016, through November 13, 2017.
Exposures: Risk factors from a questionnaire and breast density from the Breast Imaging and Reporting Data System at entry; primary risk was assessed using the Tyrer-Cuzick model.
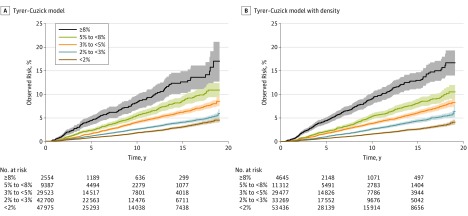
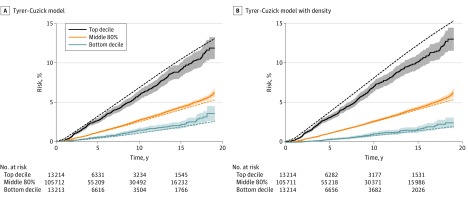
Main outcomes and measures: Incidence of invasive breast cancer was estimated with and without breast density. Follow-up began 6 months after the entry mammogram and extended to the earliest diagnosis of invasive breast cancer, censoring at 75 years of age, 2014, diagnosis of ductal carcinoma in situ, death, or health plan disenrollment. Observed divided by expected (O/E) numbers of cancer cases were compared using exact Poisson 95% CIs. Hazard ratios for the top decile of 10-year risk relative to the middle 80% of the study population were estimated. Constancy of relative risk calibration during follow-up was tested using a time-dependent proportional hazards effect.
Results: In this cohort study of 132 139 women (median age at entry, 50 years; interquartile range, 44-58 years), 2699 invasive breast cancers were subsequently diagnosed after a median 5.2 years of follow-up (interquartile range, 2.4-11.1 years; maximum follow-up, 19 years; annual incidence rate [IR] per 1000 women, 2.9). Observed number of cancer diagnoses was close to the expected number (O/E for the Tyrer-Cuzick model, 1.02 [95% CI, 0.98-1.06]; O/E for the Tyrer-Cuzick model with density, 0.98 [95% CI, 0.94-1.02]). The Tyrer-Cuzick model estimated 2554 women (1.9%) to be at high risk (10-year risk of ≥8%), of whom 147 subsequently developed invasive breast cancer (O/E, 0.79; 95% CI, 0.67-0.93; IR per 1000 women, 8.7). The Tyrer-Cuzick model with density estimated more women to be at high risk (4645 [3.5%]; 273 cancers [10.1%]; O/E, 0.78; 95% CI, 0.69-0.88; IR per 1000 women, 9.2). The hazard ratio for the highest risk decile compared with the middle 80% was 2.22 (95% CI, 2.02-2.45) for the Tyrer-Cuzick model and 2.55 (95% CI, 2.33-2.80) for the Tyrer-Cuzick model with density. Little evidence was found for a decrease in relative risk calibration throughout follow-up for the Tyrer-Cuzick model (age-adjusted slope, -0.003; 95% CI, -0.018 to 0.012) or the Tyrer-Cuzick model with density (age-adjusted slope, -0.008; 95% CI, -0.020 to 0.004).
Conclusions and relevance: Breast cancer risk assessment combining classic risk factors with mammographic density may provide useful data for 10 years or more and could be used to guide long-term, systematic, risk-adapted screening and prevention strategies.
Conflict of interest statement
Figures
Comment in
-
Competing Risks for a Diagnosis of Invasive Breast Cancer.JAMA Oncol. 2019 Jan 1;5(1):110-111. doi: 10.1001/jamaoncol.2018.5058. JAMA Oncol. 2019. PMID: 30452520 No abstract available.
-
Competing Risks for a Diagnosis of Invasive Breast Cancer-Reply.JAMA Oncol. 2019 Jan 1;5(1):111. doi: 10.1001/jamaoncol.2018.5102. JAMA Oncol. 2019. PMID: 30452738 Free PMC article. No abstract available.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. , eds. GLOBOCAN 2012: Estimated Cancer Incidence and Mortality Worldwide in 2012, version 1.0. IARC Cancer Base 11. Lyon, France: International Agency for Research on Cancer; 2013. http://globocan.iarc.fr. Accessed July 23, 2014.
-
- Massat NJ, Dibden A, Parmar D, Cuzick J, Sasieni PD, Duffy SW. Impact of screening on breast cancer mortality. Cancer Epidemiol Biomarkers Prev. 2016;25(3):455-462. - PubMed
-
- Gail MH, Brinton LA, Byar DP, et al. . Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J Natl Cancer Inst. 1989;81(24):1879-1886. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
