

All for One and One for All: Mental Disorders in One Dimension
- PMID: 29621902
- PMCID: PMC6120790
- DOI: 10.1176/appi.ajp.2018.17121383
All for One and One for All: Mental Disorders in One Dimension
Abstract
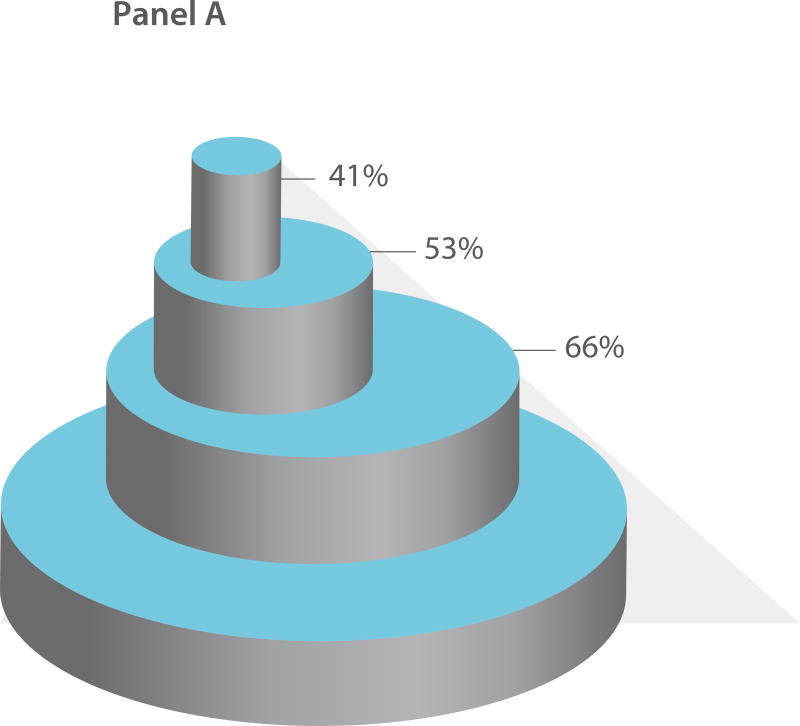
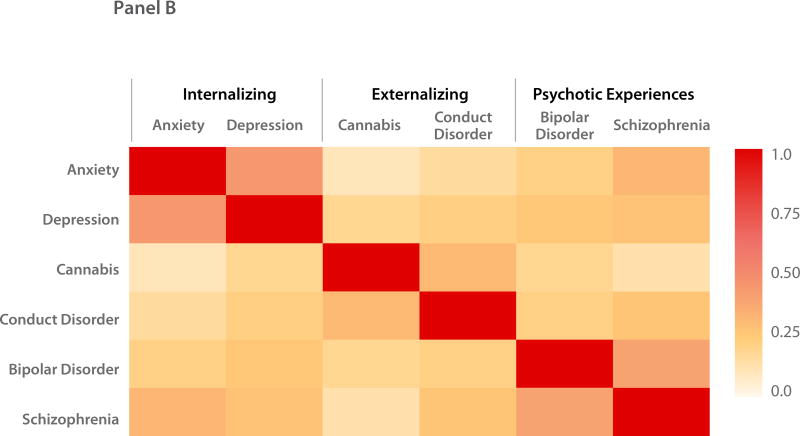
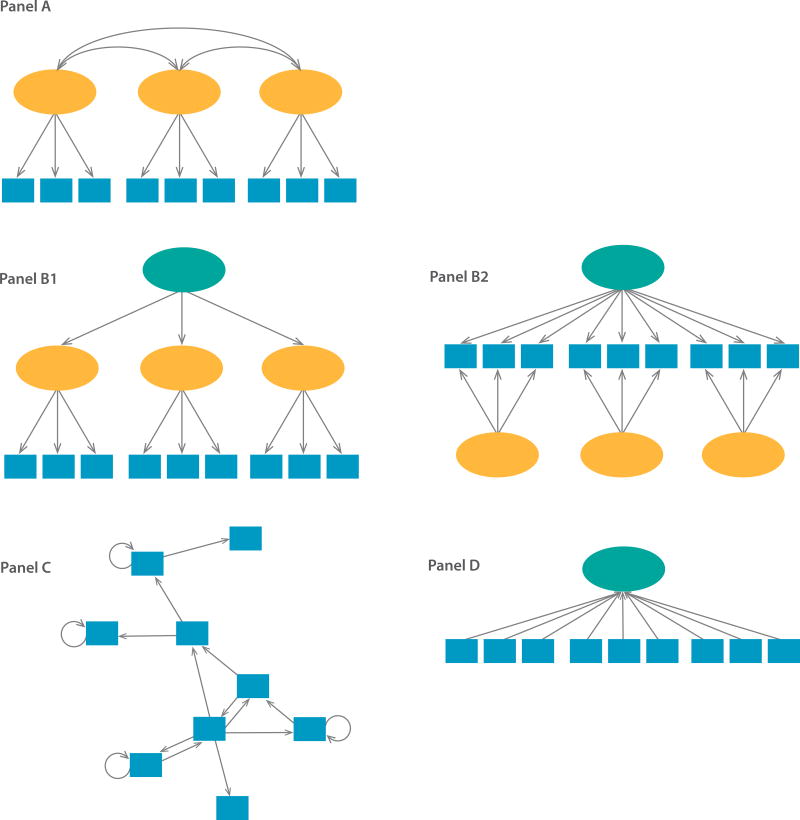
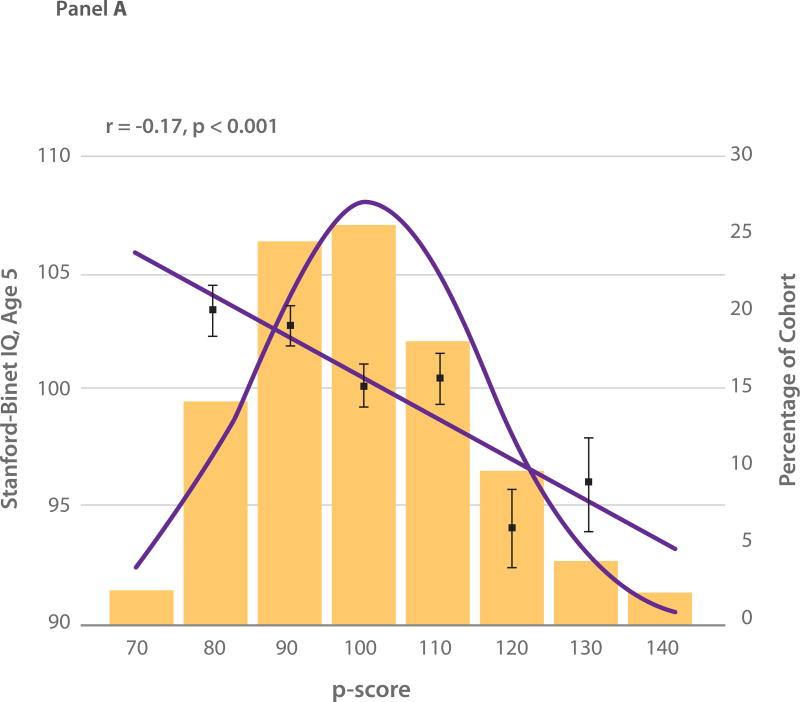
In both child and adult psychiatry, empirical evidence has now accrued to suggest that a single dimension is able to measure a person's liability to mental disorder, comorbidity among disorders, persistence of disorders over time, and severity of symptoms. This single dimension of general psychopathology has been termed "p," because it conceptually parallels a dimension already familiar to behavioral scientists and clinicians: the "g" factor of general intelligence. As the g dimension reflects low to high mental ability, the p dimension represents low to high psychopathology severity, with thought disorder at the extreme. The dimension of p unites all disorders. It influences present/absent status on hundreds of psychiatric symptoms, which modern nosological systems typically aggregate into dozens of distinct diagnoses, which in turn aggregate into three overarching domains, namely, the externalizing, internalizing, and psychotic experience domains, which finally aggregate into one dimension of psychopathology from low to high: p. Studies show that the higher a person scores on p, the worse that person fares on measures of family history of psychiatric illness, brain function, childhood developmental history, and adult life impairment. A dimension of p may help account for ubiquitous nonspecificity in psychiatry: multiple disorders share the same risk factors and biomarkers and often respond to the same therapies. Here, the authors summarize the history of the unidimensional idea, review modern research into p, demystify statistical models, articulate some implications of p for prevention and clinical practice, and outline a transdiagnostic research agenda. [AJP AT 175: Remembering Our Past As We Envision Our Future October 1910: A Study of Association in Insanity Grace Helen Kent and A.J. Rosanoff: "No sharp distinction can be drawn between mental health and mental disease; a large collection of material shows a gradual and not an abrupt transition from the normal state to pathological states."(Am J Psychiatry 1910; 67(2):317-390 )].
Keywords: Development; Diagnosis And Classification; Etiology; Transdiagnostic; p Factor.
Figures
Comment in
-
A new "inside-out" perspective on general factor p.Eur Psychiatry. 2019 Sep;61:85-87. doi: 10.1016/j.eurpsy.2019.06.009. Epub 2019 Aug 5. Eur Psychiatry. 2019. PMID: 31394486 No abstract available.
References
-
- Kotov R, Krueger RF, Watson D, Achenbach TM, Althoff RR, Bagby M, Brown TA, Carpnter WT, Caspi A, Clark LA, Eaton NR, Forbes MK, Forbush KT, Goldbers D, Hasin D, Hyman SE, Ivanova MY, Lynam DR, Markon K, Miller JD, Moffitt TE, Morey LC, Ormel J, Patrick CJ, Regier DA, Rescorla L, Robinson E, Ruggero CJ, Samuel DB, Selbom M, Simms LJ, Skodol AE, Slade T, South SC, Tackett JL, Waldman ID, Widiger TA, Wright AGC, Zimmerman M. The hierarchical taxonomy of psychopathology (HiTOP): A dimensional alternative to traditional nosologies. J Abnorm Psychol. 2017 - PubMed
-
- Wakefield JC. Diagnosticissues and controversies in DSM-5: Return of the false positives problem. Annu Rev Clin Psychol. 2016;12:105–132. - PubMed
-
- Zachar P, Kendler KS. The philosophy of nosology. Annu Rev Clin Psychol. 2017;13:49–71. - PubMed
-
- Clark LA, Cuthbert B, Lewis-Fernandez R, Narrow WE, Reed GM. Three approaches to understanding and classifying mental disorder: ICD-11, DSM-5, and the National Institute of Mental Health’s Research Domain Criteria (RDoC) Psychological Science in the Public Interest. 2017;18:72–145. - PubMed
-
- Caron C, Rutter M. Comorbidity in child psychopathology: concepts, issues and research strategies. J Child Psychol Psychiatry. 1991;32:1063–1080. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
